
There is a time and place for virtually all types of drugs, and that includes anabolic androgenic steroids. The two situations for which the use of anabolic androgenic steroids is appropriate include the following:
- Sarcopenia, in which the individual experiences in skeletal muscle mass due to aging, leading to frailty syndrome;
- Transitioning from female to male (transgender men): For individuals transitioning from female to male (transgender men), medical treatment includes hormonal therapy with testosterone.
I. Sarcopenia
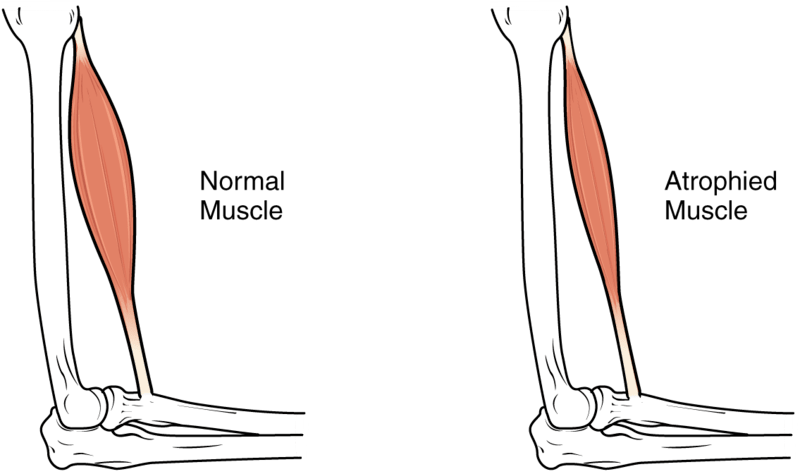
Photo from wikipedia entry entitled “Sarcopenia”, Version 8.25 from the Textbook OpenStax Anatomy and Physiology, Published 18 May 2016, Source https://cnx.org/contents/FPtK1zmh@8.25:fEI3C8Ot@10/Preface, Author OpenStax
The National Cancer Institute defines sarcopenia as “A condition characterized by loss of muscle mass, strength, and function in older adults. Signs and symptoms include weakness, fatigue, loss of energy, balance problems, and trouble walking and standing. Muscle loss or weakness can lead to falls, broken bones, and other serious injuries and can affect a person’s ability to care for oneself. Older age, getting little or no exercise, and poor nutrition may increase the risk of sarcopenia.” ( https://www.cancer.gov/publications/dictionaries/cancer-terms/def/sarcopenia)
The loss in lean mass muscle mass with ageing is due to a reduction in the number of muscle fibers and a decrease in size of the remaining fibers. Ageing is also accompanied by an accumulation of shrunken muscle fibers and an increase in muscle fat infiltration.
These changes lead to the development and progression of frailty, which is conceptualized as a vulnerability to a number of adverse outcomes such as falls, hospitalization, disability and death in older adults. The most commonly used model, focuses on physical frailty and comprises five criteria drawn from a hypothetical cycle of decline:
- Shrinking or sarcopenia
- Muscle weakness
- Slow gait speed
- Exhaustion
- Low Physical activity.
People with three or more of the above criteria are considered frail and those with one to two are considered intermediate or prefrail.
O’Connell and Wu (2014) state that the etiology (cause) of sarcopenia involves multiple mechanisms, but there is reason to believe that a major cause is the age-related decline in anabolic hormone levels, particularly testosterone.
The majority of testosterone (T) is tied up to albumin or sex hormone binding protein (SHBG) while the unbound fraction is referred to as free T. Total T levels decline modestly with age in men, while free T levels decline more steeply due to a concomitant increase in SHBG (O’Connell and Wu, 2014).
In most studies, there is a relationship between lower T levels (especially free T) and frailty. T is consistently related to muscle strength, but less clearly related to physical function.
T supplementation is associated with the following:
- Dose-dependent increases in muscle mass and reciprocal decreases in fat mass in young and older men;
- Dose-dependent improvements in muscle strength of strength and power.
The mechanisms by which these effects are achieved are through multiple cellular targets, leading to increases in the number of myonuclei (nuclei in muscle tissue) and muscle protein.
II. Transitioning from female to male (transgender men)
As an introduction to the phenomenon of transitioning from female to transgender male, it might be useful to see Jamie Wilson’s transition photos, which can be accessed via https://www.boredpanda.com/transgender-man-before-and-after-jamie-wilson/.
The National Library of Medicine defines “gender dysphoria” as the following: “Gender dysphoria (previously gender identity disorder), according to the Diagnostic and Statistical Manual of Mental Disorders, is defined as a “marked incongruence between their experienced or expressed gender and the one they were assigned at birth.” People who experience this turmoil cannot correlate to their gender expression when identifying themselves within the traditional, rigid societal binary male or female roles, which may cause cultural stigmatization. This can further result in relationship difficulties with family, peers, and friends and lead to interpersonal conflicts, rejection from society, symptoms of depression and anxiety, substance use disorders, a negative sense of well-being and poor self-esteem, and an increased risk of self-harm and suicidality. Patients with this condition should be provided with psychiatric support. Hormonal therapy and surgical therapy are also available depending on the individual case and the patient’s needs. This activity describes the evaluation and management of gender dysphoria and reviews the role of the interprofessional team in improving care for those with this condition” (https://www.ncbi.nlm.nih.gov/books/NBK532313/#:~:text=Gender%20dysphoria%20(GD)%2C%20according,termed%20%22gender%20identity%20disorder.%22).
This same website details the steps involved in the successful transitioning of a female to a transsexual male, which include the following:
Counseling:
- Adequate counseling is necessary for this population before starting treatment:
- Sexual health: incidence of sexually transmitted infections and HIV was higher in this population.
- Care team: a comprehensive approach with an endocrinologist and mental health providers should be made available.
- Expectations: transgender hormonal and surgical treatment options will help address the patient’s external appearance to be in congruence with their gender identity. Unrealistic expectations should be addressed adequately. A supportive network of peers, friends, and family is often helpful.
- Risks and benefits of treatment: both hormonal and surgical therapies accompany significant risks: venous thromboembolism, bone mineral density, and pubertal suppression.
- Fertility preservation: before initiating hormonal and surgical treatment, the patient might lose the ability to reproduce. So it is important to discuss fertility preservation by freezing the individual’s gametes.
Surgery
- The criterion is needed, in addition to those listed above, for initiating hormonal treatment before opting for surgical treatment. The individual should be on one year of continuous hormone therapy and living in the desired gender role.[11]
- This is often the last step of the treatment process. The counseling discussed above should be continued for these patients, and unrealistic expectations should be addressed. Since these are often irreversible procedures, good insight, and counseling, along with social support, are required to predict a favorable outcome.
- These surgeries are often referred to as “top surgery” and “bottom surgery.”
- For FTM: Metoidioplasty, where the clitoris is released from the ligament it is attached to, and tissue is added to increase the length and the girth. Scrotoplasty (testicular implants) and phalloplasty (penile implant) are also methods; however, the expense involved is significant, and the expertise required for these surgeries is not very common.
- In the end, constant and continued support from family, community, and peers predict favorable outcomes, even after seeking medical and mental health treatment. Individual and group therapies should be continued. Confounding substance use problems should be addressed.
Hormonal treatment
The aim is to suppress the internally produced hormones and to administer and maintain cross-sex hormones in their physiological range. There has been a great push to start hormonal therapy in these patients before they hit puberty, but it is still under research, and ethical issues persist.
Criteria for starting treatment:
- Persistent and well-documented gender dysphoria
- Capacity to consent for the treatment.
- Mental or medical underlying issues are in control.[11]
Transgender men (FTM):
Their primary treatment measure is testosterone injectables, usually scheduled once weekly (the oral route is not recommended due to the first pass through the intestines and liver). During the first few months, increased muscle mass, acne, and libido are seen, along with the cessation of menses. Eventually, more permanent changes, such as the deepening of the voice and enlarged clitoris, occur following 3 to 6 months of therapy. Routine monitoring of hemoglobin, hematocrit, liver function, cholesterol, and screening for diabetes should be done. As per Endocrine Society guidelines 2017, hematocrit or hemoglobin needs to be measured at baseline and every three months for the first year and then one to two times a year. The goal is to maintain the testosterone levels in the physiologic normal male range and avoid the adverse events resulting from excess testosterone therapy, particularly erythrocytosis, sleep apnea, hypertension, excessive weight gain, salt retention, lipid changes, and excessive or cystic acne. Measuring BMD and screening for osteoporosis is essential, especially in patients who are not compliant or are at higher risk for bone loss.[14][13]
Providers in this area of care are encouraged to start hormonal therapy before puberty for maximum results and patient satisfaction. However, parental consent for children and young adolescents for initiating hormonal therapy remains controversial. The physician should inform the patients that testosterone is teratogenic. Contraceptive methods, including IUDs, etc., should be discussed with the patients.[10]
III. Illicit use: Acquisition of muscle mass for competition or body building
The use of anabolic androgenic steroids for the treatment of sarcopenia and for facilitating FTM transitioning are medically prescribed. However, the use of these steroids to acquire muscle mass for competition constitutes an illicit use, and can lead to serious health issues.
Here, the goals are to increase lean muscle mass, reduce fat and speed up recovery from injury. The types of individuals who would use anabolic steroids include the following:
- Professional athletes and bodybuilders who are involved in competitive sport or who have a strong desire to succeed.
- People who work in industries where muscle strength is important – such as security workers, police, construction workers and defence force staff.
- Young people and adults who are concerned about their body image and want to look muscular to feel good. This may include people who work in the fashion and entertainment industries ( https://www.betterhealth.vic.gov.au/health/healthyliving/steroids ).
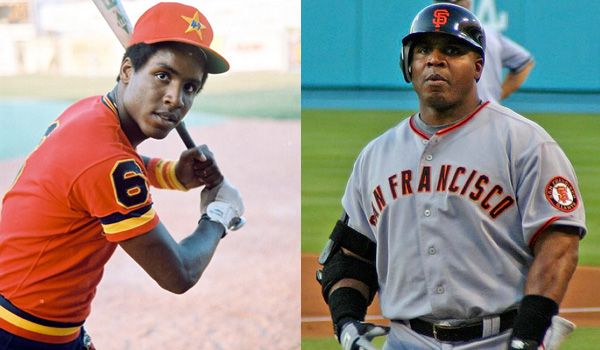
The results can be quite striking:
- L-Barry Bonds as a rookie; R-Several years later…
Female and male body builders


Police officers
In 2006, Jose Canseco wrote an expose, entitled “Juice” in which he showed just how prevalent anabolic androgenic steroids were in MBA professional baseball.
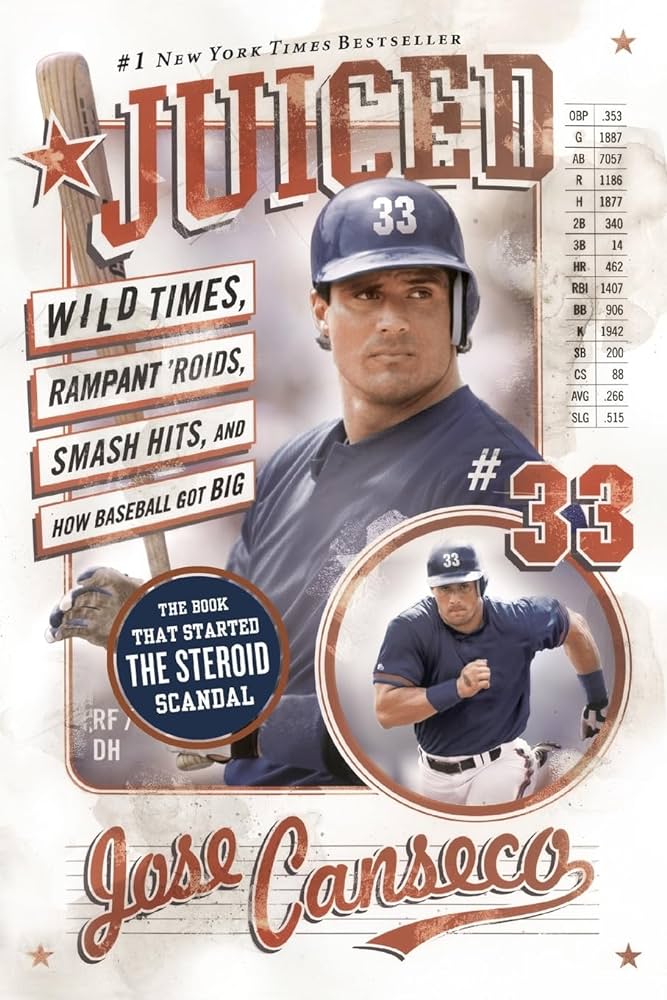
Here is a quote from that book: “The challenge is not to find a top player who has used steroids. The challenge is to find a top player who hasn’t. No one who reads this book from cover to cover will have any doubt that steroids are a huge part of baseball, and always will be, no matter what crazy toothless testing schemes the powers that be might dream up.”
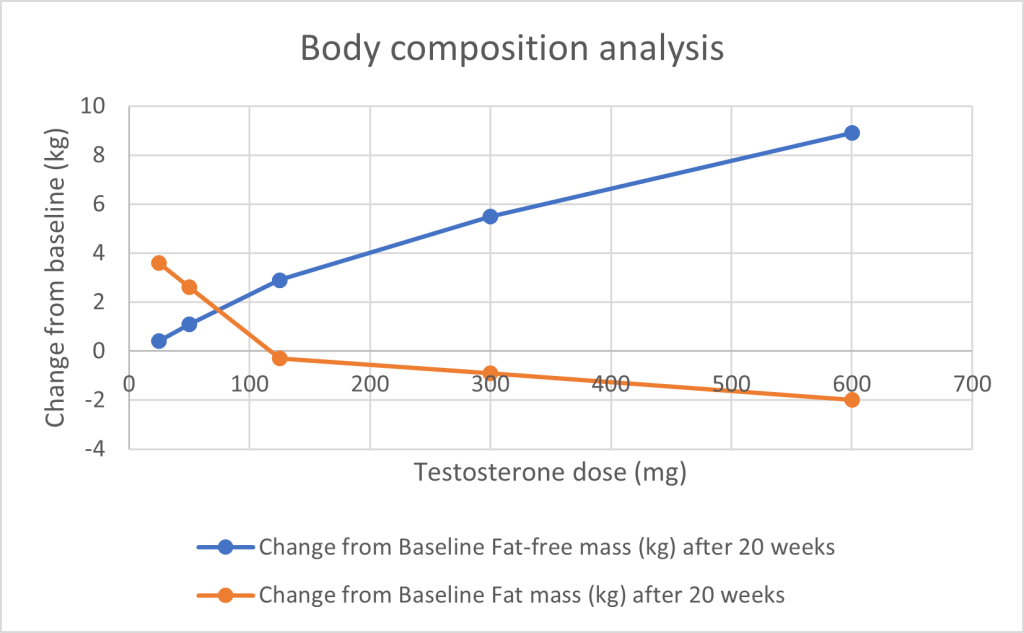
The use of steroids is quite effective in reducing fat mass, increasing fat-free (i.e. muscle mass), increasing individual muscle volume, and increasing muscle performance, even without concomitant anaerobic exercise, as seen in the following graphs, adapted from Tables 3, 4, 5 of Bhasin, et. al., (2001). In this study 61 healthy males, aged 18-35 years, were recruited to determine the effects of testosterone the above-mentioned parameters. Their endogenous testosterone production was suppressed with the monthly administration of a long-acting gonadotropin-releasing hormone (GnRH) agonist, so that the only testosterone circulating in these individuals was from their injections:
- There is a direct relationship between testosterone dose and fat-free mass, and an inverse relationship between testosterone dose and fat mass.
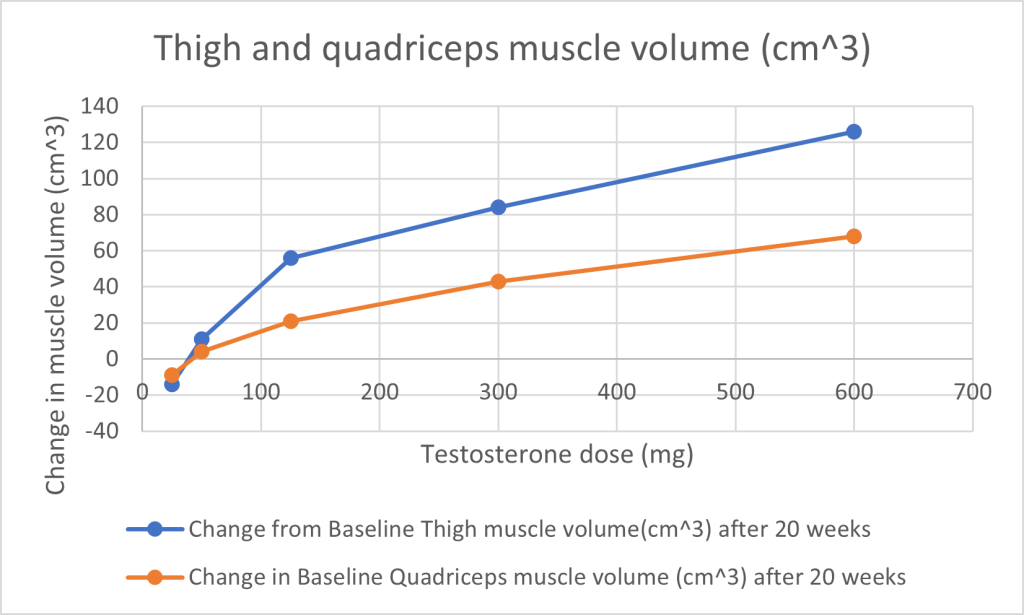
2. The two muscles which are used to measure changes in volume are the thigh and quadriceps muscle. There is a direct relationship in the increase in muscle volume with increased testosterone dose.
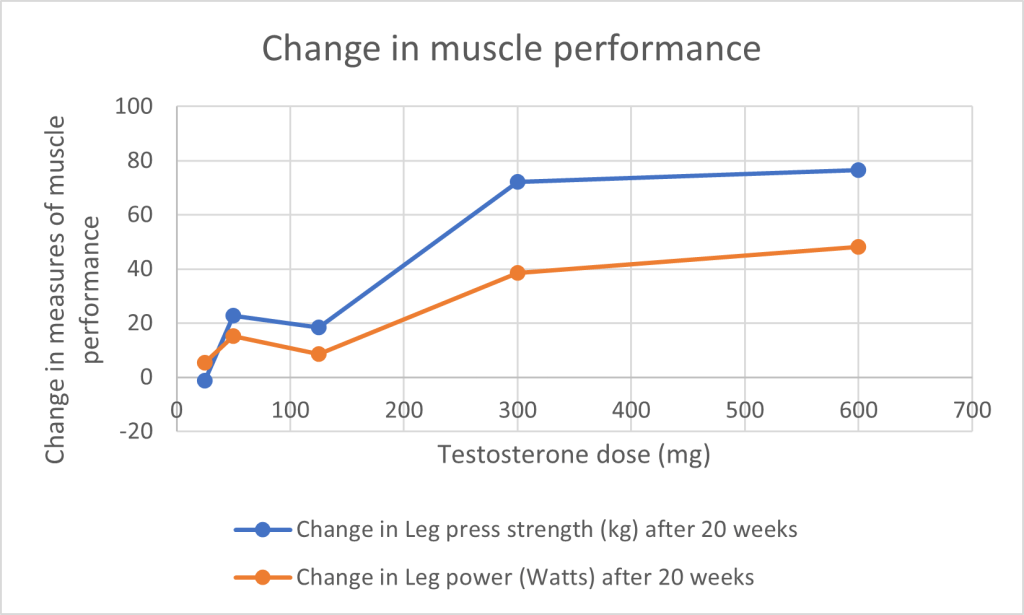
3. Both leg press strength, measured in kg, and leg power, measured in watts, increase with increased testosterone dose.
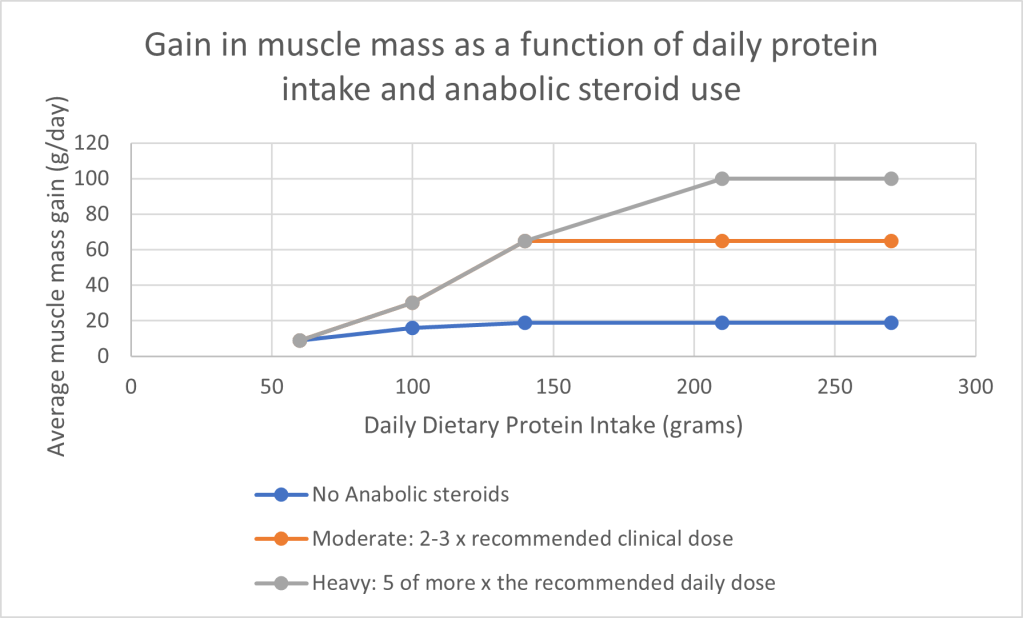
4. The potentiating effect of testosterone is increased when individuals engage in simultaneous weightlifting/anaerobic exercise. The following figure is adapted from Table 3-1 of Taylor (2002):
Using steroids for increasing muscle mass brings with it a litany of risks. The following text is taken from https://www.betterhealth.vic.gov.au/health/healthyliving/steroids .
Side effects of anabolic steroids
The effects of anabolic steroid use can differ from person to person. Some people may experience:
- fluid retention (also called water retention or oedema)
- difficulty sleeping
- damage to nerves from injecting steroids
- irritability, mood swings, aggression or depression
- increased sex drive (libido)
- skin changes – acne that results in scarring
- more colds.
Men may experience:
- testicle and penis shrinkage*
- reduced sperm count
- erectile dysfunction (or impotence)
- prostate problems
- gynaecomastia (breast development)
- baldness (patterned hair loss)
- involuntary and long-lasting erection.
*Q: How do you measure testicle shrinkage?
A: Why, with an orchidometer, of course. An orchidometer is a necklace-like string of beads of increasing size, as shown in the following illustration:

Women may experience:
- irregular menstrual cycle or loss of periods (amenorrhoea)
- shrunken breasts
- deepened voice
- facial and body hair growth (such as hirsutism)
- abnormal growth of the clitoris.
Young people may experience:
- stunted growth
- premature balding
- acne scarring
- injury caused by excessive, intense workouts
- stretch marks on the chest and arms
- prematurely aged (or ‘leathery’) skin.
Long-term effects of anabolic steroids
Anabolic steroids can produce many unpleasant and often permanent side effects, including:
- damage to the gonads (testicles or ovaries)
- liver disease
- malfunctions of the kidneys, liver or heart
- ‘roid rage’, which is characterised by uncontrollable outbursts of psychotic aggression
- paranoia and mood swings, including deep depression
- severe acne, which can cause scarring
- high blood cholesterol levels
- high blood pressure (hypertension)
- injuries to tendons that can’t keep up with the increased muscle strength
- delusional feelings of being superhuman or invincible.
- trembling and muscle tremors.
- nerve damage from needle use – this may lead to conditions such as sciatica
- unsafe needle use can increased the risk of contracting infactions such as hepatitis B and C, HIV and tetanus.
Dependence on anabolic steroids
Anabolic steroids do not cause physical dependence. However, if a person relies on them for their self-esteem and confidence, then giving up can be extremely difficult. The pressure to keep using steroids may result in feelings of anger or depression if their access to steroids is denied, even temporarily.
Withdrawal from anabolic steroids
It can take up to 4 months to restore natural testosterone levels after being on anabolic steroids for a long time. Withdrawal symptoms from steroids can include:
- fatigue
- weight loss due to lowered appetite
- decreased strength
- depression.
Treatment for anabolic steroid addiction
Treatment options for drug dependence or addiction may include:
- detoxification
- individual counselling
- group therapy.
Peer support – or talking to someone who has been in the same situation – can also be helpful.
See your doctor for information and referral, or contact an alcohol and other drug service in your area.
Canseco, J. (2006), Juiced. It Books.
O’Connell, M.D.L.; Wu, F.C.W. (2014). Androgen effects on skeletal muscle: implications for the development and management of frailty. Asian Journal of Andrology 16:203-212. doi: 10.4103/1008-682X, 122581.
Shalender, B.; Woodhouse, L.; Casaburi, R.; Singh, A.B.; Bhasin, D.; Berman, N.; Chen, X.; Yarasheski, K.E.; Magliano, L.; Dzekov C.; Dzekov, J.; Bross, R.; Phillips, J.; Sinha-Hikim, I.; Shen, R.; Storer, T.W. (2001). Testosterone dose-response relationships in healthy young men. Am. J. Physiol. Endodrinol. Metab. 281:E1172-E1181.
Taylor, W.N. (2002). Anabolic Steroids and the Athlete, 2nd edition. McFarland & Company, Inc., Publishers, Jefferson, N.C.
