
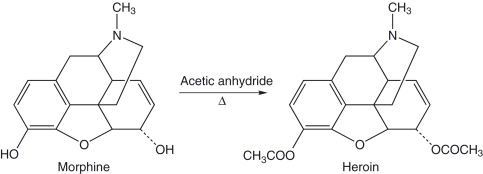
Fentanyl is an opioid, a chemical that acts on the same brain receptors as opiates, but lacks the chemical backbone that opiates do. For example, here is an illustration of morphine and heroin, and you can see that the backbone of these two compounds is identical:
What opioids have in common
Pharmacological effects
Pharmacological effects include the following:
- Analgesia: There is no loss of consciousness, nor does not affect other modalities. The pain may persist, but the patient/user feels “comfortable”, and tolerates the pain;
- Euphoria: There is a strong feeling of contentment, well-being and lack of concern, which is part of the affective, or reinforcing response of drug. Opioid use becomes an acquired drive state that permeates all aspects of human life, and is often described in ecstatic and sexual terms, although euphoria declines with frequent use. The mechanism of morphine’s positive reinforcing and euphoria-producing action probably involves more than mu receptors, especially the dopaminergic neurons. In the ventral tegmental area, morphine inhibits GABA neurons via mu-opioid receptors, thus disinhibiting dopaminergic neurons and increasing dopamine input in the nucleus accumbens and in other areas. This may be involved in the mechanism of reward
- Sedation and anxiolysis: Sedation is not as deep as that produced by CNS depressants. “Mental clouding” is prominent, which is accompanied by a lack of concentration, apathy, complacency, lethargy, reduced mentation, and a sense of tranquility. These actions probably follow from mu receptor inhibition of neuronal activity in the locus coeruleus, the principal clustering of norepinephrine neurons in the brain;
- Depression of Respiration: The use of morphine decreases the respiratory center’s sensitivity to higher levels of carbon dioxide in blood. Respiratory rate is depressed even at therapeutic doses, and the depression of respiration can be fatal, especially if alcohol or other sedatives are taken simultaneously. The depression of respiration by the combination of alcohol or sedatives taken with morphine is synergistic;
- Nausea and vomiting: The chemoreceptor trigger zone, located in the medulla, is stimulated by morphine. Stimulation of the trigger zone by morphine will induce nausea and vomiting. Although the symptoms are unpleasant, they are not life-threatening;
- Gastrointestinal symptoms: Intestinal tone increases, motility decreases, feces dehydrate, and intestinal spasms (cramping) occur. All this tends to constipate people. Tolerance to the constipating qualities of opioids does not occur, so drug-dependent individuals have a problem with constipation. Two opioids have been developed that only VERY minimally cross blood-brain barrier, hence they are very good opioid antidiarrheals with no analgesic action – Lomotil and Imodium;
- Other effects of morphine: Morphine suppresses the cough center, located in brain stem. Furthermore, it induces significant constriction of the pupils, manifesting itself as miosis, as shown in this person’s left eye:

Mode of action
Opioids exert at least part of their analgesic action by inhibiting the release of substance P, a neuropeptide 11 amino acids in length, which transmits nociceptive information from the site of injury to the spinal cord. Its release in the dorsal horn of the spinal cord is typically regulated intrinsically by endogenous endorphins.
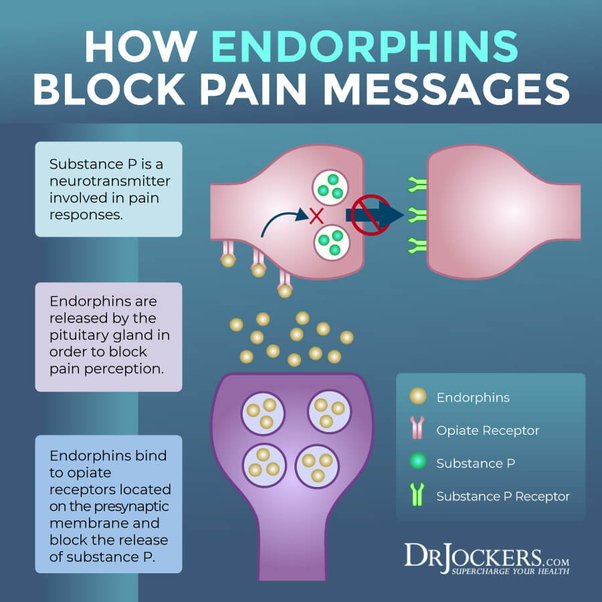
The perception of pain is caused by the activation of small-diameter (afferent) fibers of peripheral nerves. Nociceptive neurons originate in peripheral tissues, e.g. skin, muscle, viscera, and can be activated by mechanical, thermal, chemical, and injury. Action potentials are conducted to terminals in the dorsal horn of the spinal cord where substance P is released.
When substance P is released, it activates other spinal cord neurons which, in turn, transmit information about noxious stimuli to the brain via the spinothalamic tract and the spinoreticular tract. Opioid receptors are also found in the thalamus, brain stem, and limbic system. Two descending pathways, which originate in the lower brain stem, modulate the transmission of pain impulses by activating pain-inhibitory systems. Activation of either pathway, which consist of descending NE and serotonin-releasing neurons, activates endorphin neurons in the dorsal horn of the spinal cord, which in turn, exerts an analgesic action by further inhibiting substance P release. The affective component of pain is the component that determines our emotional response by reducing the distress associated with pain.
Fentanyl, like opiates, causes the increase of the neurotransmitter dopamine (Da) in the reward areas of the brain, which elicits the stereotypical exhilaration and relaxation effects, and is typically associated with the addiction to the drug.
However, as an analgesic, fentanyl is far more potent than morphine. In fact, it is typically 50 to 100 times more potent. A dose of only 100 micrograms can produce equivalent analgesia to approximately 10 mg of morphine (Ramos-Matos, et. al. 2023). In fact, 2 milligrams, the equivalent of a few grains of salt, can be fatal.
The shift away from heroin to fentanyl has led to a terrible epidemic whose effects are visible on the streets of San Francisco:


In the pictures shown above, you’re seeing people bent over in an extreme position called the “fentanyl fold”, indicating that (s)he has just taken a dose. Sometimes, people remain in this posture frequently enough and for such extended periods of time that their posture can be permanently damaged (Langer and Chen, 2023).
Langer, M-A, L.; Chen, M.K. (2023). Fentanyl is destroying San Franciso’s soul. https://www.nzz.ch/english/fentanyl-is-destroying-san-franciscos-soul-ld.1749900
Ramos-Matos, C.F.; Bistas, K.B.; Lopez-Ojeda, W. (2023). Fentanyl: StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK459275/
