
Image from https://wbkhealth.com/why-mental-health-disorders-co-exist-with-substance-use/
The number of people who use, and misuse alcohol, cannabis, and illicit drugs is, in fact, quite high. The National Center for
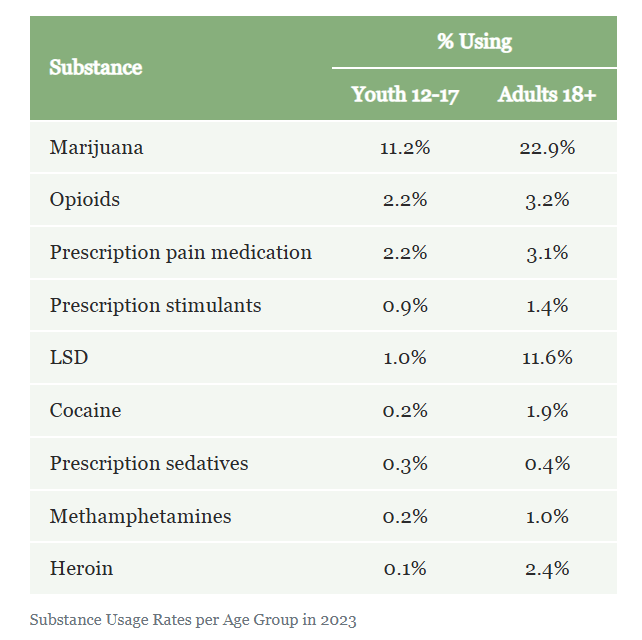
Drug Abuse Statistics maintains a website, https://drugabusestatistics.org/, which details the numbers and percentages of people who use illicit drugs such as marijuana (cannabis), cocaine, ecstasy, methamphetamine, LSD, heroin, and other opioids. The following table appears on that website:
Research shows that individuals with mental health conditions are at increased risk of developing substance use disorder (Anderer and Rekito, 2025). Such people often self-medicate with drugs or alcohol.
In their survey, they report that mental health conditions were linked with binge drinking. In the case of adolescents who’d had a recent major depressive episode or experienced moderate to severe anxiety, 6% binge drank, compared with 3% or less of those who didn’t report a mental health issue. With adults, 30% of all adults with any level of mental illness reported binge drinking.
Mental health conditions are particularly linked with increased binge drinking and with increased drug usage. For example, of adolescents who have had a recent major depressive episode or experienced moderate to severe anxiety, 6% binge drink, compared with 3% or less of those who didn’t report a mental health issue.
Furthermore:
- Nearly 30% of all adults with any level of mental illness reported binge drinking;
- About 3 in 10 adolescents who have had a major depressive episode used substances compared with 1 in 10 who hadn’t had one;
- A quarter of those with moderate or severe anxiety used drugs compared with 10% of those without anxiety.
Scientists theorize that much of the excessive alcohol or drug use by these individuals is driven by an attempt to self-medicate and thereby reduce the negative affect of these conditions, which include the following:
- Schizophrenia: Schizophrenia is characterized by persistent delusions, hallucinations, disorganized speech, disorganized behavior, and negative symptoms such as the absence of emotional expression or lack of motivation or initiative (American Psychiatric Association, 1994). Data generated from the Epidemiologic Catchment Area study has demonstrated that over a 1/3 of people with a diagnosis of either schizophrenia or schizophreniform disorder (a related, but less severe disorder lasting less than 6 months) also met the criteria for an AUD diagnosis at some time during their lives, and nearly 50% met the criteria for any substance use disorder, excluding nicotine dependence (Drake and Mueser, 2002);
- Bipolar disorder: Bipolar disorder, also called manic depression, is a mood disorder characterized by extreme fluctuations in mood from euphoria to severe depression, interspersed with periods of normal mood (i.e. euthymia) (Sonne and Brady, 2002). Bipolar I disorder, bipolar II disorder, and cyclothymia are included within this classification, of which bipolar I disorder is the most severe. Given its severity, the prevalence of alcohol dependence among individuals with bipolar I disorder is particularly high (31.5%) (See Table I below);
- Childhood antisocial behavior (conduct disorder and oppositional defiant disorder): Antisocial behaviors are acts which violate social rules and basic rights of others, and “childhood” refers to ages 12 and younger. The DSM-IV criteria for conduct disorder (CD) include “aggression toward people and animals, destruction of property, deceitfulness, theft, and other serious social rule violations”, while oppositional defiant disorder (ODD) is characterized by “negativistic, hostile, and defiant behaviors, such as losing one’s temper, arguing, defying rules, deliberately annoying others, blaming others for one’s behavior, and displaying anger or vindictiveness” (Clark, Vanyukov, and Cornelius, 2002). ODD often precedes CD, and both are predictive of initiation of regular alcohol use in early adolescence.
- Attention Deficit Hyperactivity Disorder (ADHD): As a childhood mental health disorder, ADHD is characterized by inattention, impulsivity and hyperactivity (Smith, Molina, and Pelham, 2002). Three forms of ADHD are recognized, including ADHD, predominantly inattentive subtype (ADHD-IA), ADHD, predominantly hyperactive/impulsive subtype (ADHD-HI), and ADHD, combined inattentive and hyperactive/impulsive subtype (ADHD-C). ADHD affects between 3 to 7% of children in the United States, and is estimated to occur among 2 to 5% of adults in the general population. The rates of ADHD among adolescents and adults undergoing treatment for alcohol and other drug abuse is much higher – the prevalence of ADHD among adolescent patients undergoing AOD treatment is 30%, while the prevalence among adult patients is 25%;
- Social anxiety disorder: Social anxiety disorder is defined as excessive fear in social situations in which the person believes he or she will do something embarrassing or have anxiety symptoms (e.g., blushing or sweating) that will be humiliating (Book and Randall, 2002). People with this disorder tend to isolate themselves in order to avoid feared situations. According to data collected for the Epidemiologic Catchment Area and subsequent National Comorbidity studies, the prevalence of social anxiety disorder in the United States is approximately 2 to 13%. However, 15% of people receiving treatment for alcoholism also have social anxiety disorder, and AUDs are found among patients being treated for social anxiety disorder;
- Concurrent tobacco dependence or pathological gambling: Tobacco use and pathological gambling are both closely linked to alcohol consumption. For example, according to American Lung Association data, approximately 23% of adults in the United States are current smokers. Smoking rates among alcoholics, however, are estimated to be as high as 90%, with approximately 70% of alcoholics smoking at least one pack of cigarettes per day (Drobes, 2002). Pathological gambling (PG) is characterized by a persistent maladaptive pattern of gambling behavior (Grant, Kushner, and Kim, 2002). Studies in the United States have shown that 44% of those individuals with disordered gambling behavior also report a lifetime history of AUD (Cunningham-Williams, et. al., 1998).
Table I. Comorbid mood disorders, including depression and bipolar disorder, and substance abuse. (Adapted from Sonne and Brady, 2002).
| Any substance abuse or dependence (%) | Alcohol dependence | Alcohol abuse (%) | |
| Any Mood Disorder | 32.0 | 4.9 | 6.9 |
| Any Bipolar Disorder | 56.1 | 27.6 | 16.1 |
| *Bipolar I | 60.7 | 31.5 | 14.7 |
| *Bipolar II | 48.1 | 20.8 | 18.4 |
| Unipolar Depression | 27.2 | 11.6 | 5.0 |
********************************************************
In a study published earlier this year, Hyatt et. al. report a sharp increase in cannabis use after recreational cannabis legalization among individuals individuals with psychosis by a greater amount than in the general population. The study sample consisted of 1856 individuals with a lifetime history of psychosis, with a mean age of 36.6 years. This increase in cannabis use among vulnerable individuals should be a concern for regulators and legislators.
********************************************************
At the same time, the absence of a comorbid disorder may be indicative of a resilience or ability to overcome an addiction. For example, the United States military was expecting an epidemic of heroin dependence among veterans returning from Vietnam. An estimated 45% of soldiers who served in 1970-71 tried heroin, and half of them became addicted, and only 2% received treatment. However, when those soldiers returned to the United States, relatively few of them (<15%) continued to be addicted or became addicted in the 3 years after their return. Furthermore, the relapse rate among treated veterans was higher than for untreated veterans. Lee Robins, one of the authors of the original study, reevaluated her findings for the British journal Addiction, and stated that it was the availability of heroin that made narcotic use and narcotic addiction so common, that those with a history of deviant behavior before Vietnam were particularly at risk, and that addiction was rare and brief after return even when men continued to use narcotics. Apparently, the departure from the drug-saturated, stressful environment of the Vietnam War was sufficient to convince most soldiers to discontinue their use of heroin. This conclusion is all the more surprising since heroin is supposed to be one of the most addicting drugs.
American Psychiatric Association (1994). Diagnostic and Statistical Manual of Mental Disorders, (DSM-IV) 4th edition. American Psychiatric Association, Washington, D.C.
Anderer, S.; Rekito, A. (2025). Mental Health and Substance Use Linked in New Survey. Journal of the American Medical Association 334(16):1414-1415. doi:10.1001/jama.2025.15338.
Book, S.W.; and Randall, C.L. (2002). Social Anxiety Disorder and Alcohol Use. Alcohol Research & Health 26(2):130-135.
Cunningham-Williams, R.M.; Cottler, L.B.; Compton, W.M.; Spitznagel, E.L. 1998). Taking chances: Problem gamblers and mental health disorders – results from the St. Louis Epidemiologic Catchment Area (ECA) study. American Journal of Public Health 88:1093-1096.
Drobes, D.J. (2002). Concurrent Alcohol and Tobacco Dependence. Alcohol Research & Health 26(2):136-142.
Hyatt, A.S.; Flores, M.W.; Johnson, J. (2026). Cannabis Use Among Individuals With Psychosis After State-Level Commercial Cannabis Legalization. JAMA Psychiatry 83(1):74-77. doi:10.1001/jamasychiatry.2025.2539.
Smith, B.H.; Molina, B.S.G.; Pelham, W.E., Jr. (2002). The Clinically Meaningful Link Between Alcohol Use and Attention Deficit Hyperactivity Disorder. Alcohol Research & Health 26(2):122-129.
Sonne, S.C.; and Brady, K.T. (2002). Bipolar Disorder and Alcoholism. Alcohol Research & Health 26(2):103-108.
P.S.: Two interesting versions of the same song, Hurt:
First, the original:
Now, Johnny Cash’s cover, which he did late in life:
Anderer, S.; Rekito, A. (2025). Mental Health and Substance Use Linked in New Survey. Journal of the American Medical Association Data Briefr 334(16):1414-1415.


