
The deleterious effects of smoking tobacco have been known for several decades, and served as the basis for a massive lawsuit ( https://www.fightcancer.org/what-we-do/big-tobacco-lawsuit ).
With greater acceptance of the presumptive benefits of cannabis, more states and countries are legalizing cannabis for both medical and recreational purposes. As a result, there is a growing body of evidence that shows the harmful effects of cannabis smoke as well. This was, in fact, the topic of the previous blog,
My original intent in writing this blog was to show the plethora of compounds synthesized by Cannabis sativa which have therapeutic applications, and contrast that plethora with the only compound synthesized by tobacco leaves that has any practical use, nicotine, which has been used for centuries as an insecticide (https://jpds.co.in/wp-content/uploads/2019/07/12.-Rohit-Rana-799.pdf ). To my surprise, bioactive compounds found in tobacco leaves have beneficial anti-inflammatory, antitumor, antibacterial and antioxidant properties (Zou, et. al., 2021), which we will explore below.
We will then look at the compounds synthesized by Cannabis sativa to determine their therapeutic effects and applications.
I. Therapeutic compounds extracted from tobacco plants
As mentioned earlier, Zou et. al. (2021) list several classes of compounds which have therapeutic applications:
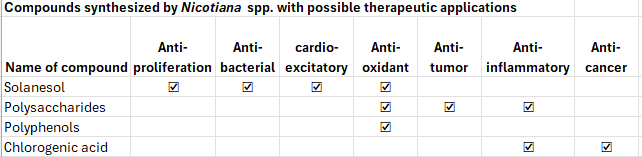
Granted, some polyphenols are toxic.
They have found that the leaves of one species, Nicotiana rusticas, are applied “for bronchitis, tonsillitis, wounds, wore throat, and arthritis. Meanwhile, its extract could also be applied as a toothache remedy, and effective to respiratory tract diseases.” Furthermore, “leaves of Nicotiana tabacum have similar functions and [are] still effective on digestive system disorders, skin illness, sinusitis, and to cure stomach infections.”
Prommaban et. al. (2022) also demonstrate antihyaluronidase and antityrosinase activity in nicotine extracts, both of which have possible applications in cosmeceutical industries. Cosmeceuticals, in turn, “represent a new category of products
placed between cosmetics and pharmaceuticals that are
intended for the enhancement of both the health and beauty of
skin (Martin and Glaser, 2011).”
The antihyaluronidase activity of tobacco extracts helps in maintaining skin hydration and tissue homeostasis by preventing the degradation of hyaluronic acid, a component of epidermis and dermis, by hyaluronidase. This activity would, in turn, prevent the aging of skin.
The antityrosinase activity would have application in the cosmetic industry, since it inhibits tyrosinase, an enzyme for the formation of melanin, a skin pigment. Tyrosinase inhibitors, mediating antityrosinase activity, therefore would serve as skin whitening agents. (Writing this last sentence reminds me of the models who served as backup to Robert Palmer’s Addicted to Love and Simply Irresistible🙂
Don’t believe me? Please see Exhibit A below:
An early P.S.: What Robert Palmer was trying to accomplish with the makeup for the models in these two videos:
Robert Palmer’s goal for the models’ makeup in the “Addicted to Love” video was to create a glamorous, fierce, and iconic 80s aesthetic inspired by Patrick Nagel‘s artwork, resulting in a sophisticated, almost “mannequin-like” look with dramatic smoky eyes, defined brows, contoured cheeks, and vibrant red lips that served as a perfect, eye-catching unit to complement the striking visuals of the video. (To see some of Patrick Nagel’s artwork, please see https://patricknagel.com/ or https://villagegallery.com/gallery/vintage-artwork/patrick-nagel/.)
III. Cannabinoids exert their effects by binding to one of two types of receptors, the CB1 and CB2 receptors.
Most CB1 receptors are located in the brain, while CB2 receptors are found throughout the body, as shown in the following image:
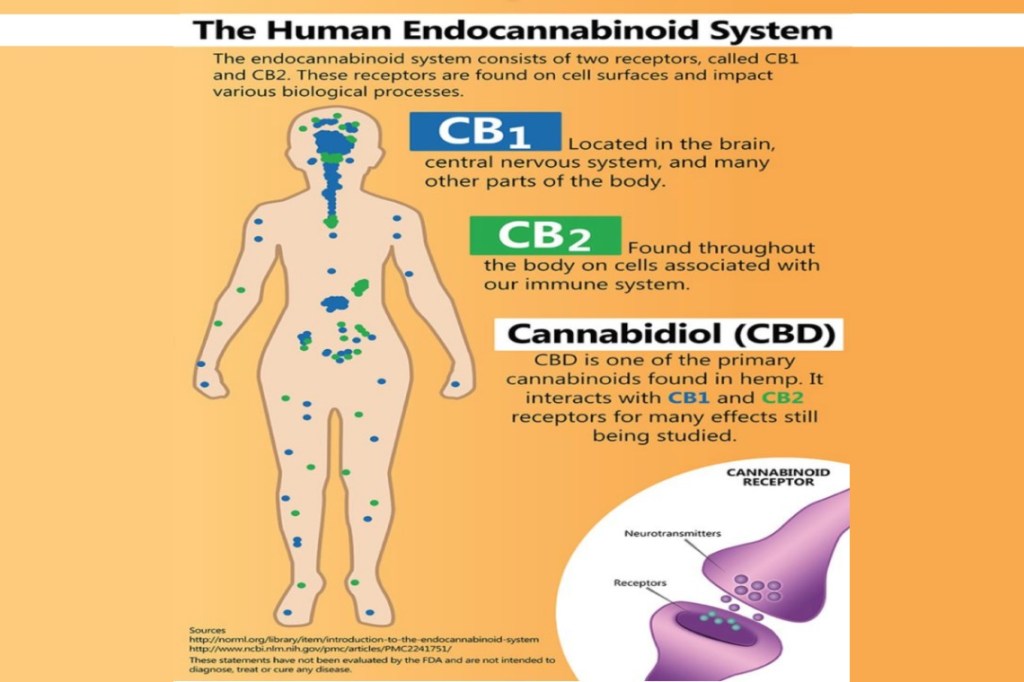
Above image extracted from https://www.pensummed.pro/blogs/cannabinoids-a-stem-cell-stimulator .
We will find that the binding of cannabinoids to these receptors results in the therapeutic properties which are shown below.
II. Therapeutic compounds extracted from cannabis plants
The following table of major secondary metabolites of Cannabis sativa and their therapeutic properties is adapted from Table 3 of Lowe, et. al. (2021):
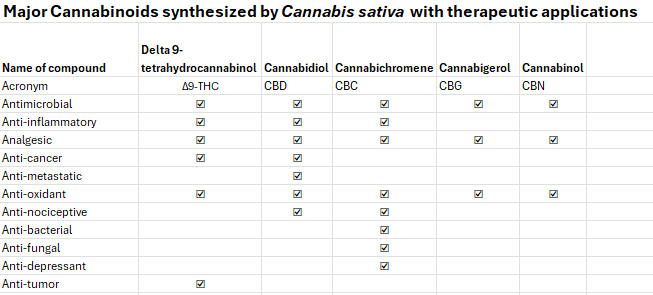
In addition to the cannabinoids listed above, there are terpenes and flavonoids which have additional neuroprotective, angiogenic, anxiolytic, and antiviral properties.
III. Therapeutic applications:
The number of drug formulations which have passed the rigorous tests and criteria of the FDA are relatively limited (see Section IV below), so there is considerable concern about standardization, dosing, potential side effects, and long-term safety (Leinen, et. al., 2023). Nonetheless, there are numerous studies that show how cannabinoids can hold great promise in the treatment of numerous conditions:
- Dental issues: Given the activity of cannabinoids on its receptors in the mouth, they may have potential therapeutic applications in the treatment of Burning Mouth Syndrome, dental caries, dental anxiety (the fear of undergoing treatment by a dentist), and periodontal disease (Lowe, et. al., 2021);
- Currently, there are a number of cannabinoid-based pharmaceuticals, including CBD-infused toothpastes, CBD Oral Sprays, CBD-infused mouthwashes, CBD chewing gum, and CBD-infused dental fillings. These products are primarily used as analgesics to provide relief from tooth pain and gum soreness, and as anti-microbials and antiseptic agents to maintain oral hygiene. However, these products have not undergone rigorous testing, and do not have FDA approval;
- Even so, cannabinoids have also been shown to be more effective in reducing bacterial colony count in dental plaques when compared to Colgate and Oral B (Stahl and Vasudevan, 2020);
- Multiple sclerosis: Multiple sclerosis (MS) is a chronic neurological autoimmune disorder, meaning that the immune system, which normally protects us from viruses and bacteria, mistakenly attacks healthy cells. In the case of MS, the immune system attacks myelin in the central nervous system. Myelin is a mixture of protein and fatty acids that makes up the protective cover (known as the myelin sheath) that coats nerve fibers (axons). In addition to causing damage to the myelin sheath, MS also damages the nerve cell bodies, which are found in the brain’s gray matter, as well as the axons themselves. As the disease progresses, the outermost layer of the brain, called the cerebral cortex, shrinks. This process is known as cortical atrophy ( https://www.ninds.nih.gov/health-information/disorders/multiple-sclerosis#:~:text=Multiple%20sclerosis%20(MS)%20is%20a,ages%20of%2020%20and%2040.) Nabiximols (Sativex) is an oromucosal spray containing equal volumes of THC and CBD, and it is used as an add-on treatment for unresponsive spasticity in multiple sclerosis patients (Bukowska, 2024);
- Alzheimer’s Disease: Alzheimer’s disease is a brain disorder that slowly destroys memory and thinking skills and, eventually, the ability to carry out the simplest tasks. People with Alzheimer’s also experience changes in behavior and personality (https://www.alzheimers.gov/alzheimers-dementias/alzheimers-disease) . The causes of Alzheimer’s disease are not yet fully understood, but probably include a combination of the following: a) Age-related changes in the brain, like shrinking, inflammation, blood vessel damage, and breakdown of energy within cells, which may harm neurons and affect other brain cells; b)Changes or differences in genes, which may be passed down by a family member. Both types of Alzheimer’s — the very rare early-onset type occurring between age 30 and mid-60s, and the most common late-onset type occurring after a person’s mid-60s — can be related to a person’s genes in some way. Many people with Down syndrome, a genetic condition, will develop Alzheimer’s as they age and may begin to show symptoms in their 40s; c)Health, environmental, and lifestyle factors that may play a role, such as exposure to pollutants, heart disease, stroke, high blood pressure, diabetes, and obesity. Cannabis significantly reduces the brain inflammation implicated in Alzheimer’s Disease. Furthermore, administration of THC and cannabidiol (CBD) together are shown to preserve memory;
- Parkinson’s Disease: Parkinson’s disease (PD) is a progressive movement disorder of the nervous system. It is associated with the progressive death of dopaminergic neurons in the substantia nigra of the brain, leading to symptoms that include problems with movement, tremor, stiffness, and impaired balance ( https://www.ninds.nih.gov/health-information/disorders/parkinsons-disease). According to Gabarin, et. al. (2023), there is no scientific evidence recommending the use of cannabis in PD patients, but there are studies that show that the symptoms associated with PD, such as tremor, anxiety, and pain, respond to cannabis use;
- Chronic neuropathic pain: Chronic neuropathic pain is a pathological condition that is difficult to treat. However, clinical studies have shown that products containing natural or synthetically produced cannabis compounds have significant analgesic properties.
- For example, Leinen, et. al. (2023) mention one study involving 338 patients with various chronic pain conditions in which a cannabis flos decoction as a supplementary treatment over 12 months was investigated. In this study, patients showed significant improvements in pain intensity, pain disability, anxiety and depression compared to their status at the beginning of the study;
- A separate observational study involving 428 individuals with osteoarthritis, autoimmune arthritis or rheumatoid arthritis showed that many participants experienced enhanced pain relief from CBD usage;
- Skin diseases: There is a growing number of pre-clinical and clinical studies dedicated to exploring the potential of cannabinoids to treat dermatologic conditions (Yoo and Lee, 2023). Because of their anti-inflammatory properties, cannabinoids are effective in the treatment of numerous dermatological pathologies, including acne vulgaris, allergic contact dermatitis, eczema, pruritus, psoriasis and skin cancer;
- Allergic Contact Dermatitis: CBD demonstrates a dose-dependent inhibition of monocyte chemotactic protein 2, which attracts mast cells and macrophages to inflammatory sites. Furthermore, it suppresses the release of pro-inflammatory cytokines. An observational study demonstrated that the topical application of CBD gel reduced a patient-oriented eczema measurement score from 16 to 8.1, a significant reduction. THC also decreases certain pro=inflammatory mediators;
- Pruritis: THC has been shown to be an effective treatment for itching in several studies. In case reports, patients with epidermolysis bullosa who were treated sublingually with CBD and THC reported improved pain scores. Patients with intractable cholestatic-related pruritis benefited from oral administration of 5 mg of THC;
- Psoriasis: Cannabinoids inhibit the release of inflammatory cytokines such as IL-2, TNF-alpha, and IFN-gamma, both of which are important in the development of psoriasis. CBD, in particular, inhibits a factor, MMP9, which degrades the extracellular matrix which holds skin together. In one split-body, double-blind, placebo-controlled study of 51 patients with mild plaque-type psoriasis, patients applied 2.5% CBD ointment and placebo twice daily for 12 weeks and showed significantly lower Psoriasis Severity Index scores on the CBD side throughout the follow-up period;
- Skin aging: Both THC and CBD stimulated cell growth in a dose-dependent manner while significantly decreasing senescence. In a separate study involving a scratch assay, both THC and CBD significantly improved wound healing in both healthy and stress-induced premature senescent skin fibroblasts.
- Amyotrophic lateral sclerosis: Amyotrophic lateral sclerosis (ALS) is a fatal type of motor neuron disease. It causes progressive degeneration of nerve cells in the spinal cord and brain. It’s often called Lou Gehrig disease after a famous baseball player who died from the disease. ALS is one of the most devastating types of disorders that affect nerve and muscle function (https://www.hopkinsmedicine.org/health/conditions-and-diseases/amyotrophic-lateral-sclerosis-als ). An online survey on the use of cannabis among such patients showed that almost 22% of respondents had improvements in motor (rigidity and cramps) and non-motor (sleep quality, pain, emotional state, quality of life and depression) symptoms;
- Parkinson’s Disease: Parkinson’s Disease (PD) is a progressive neurodegenerative disease, characterized by the death of dopamine-releasing neurons in a part of the brain called the substantia nigra. The ensuing reduction in dopamine levels in the brain lead to the major symptoms of PD, such as slowness of movement (bradykinesia), stiffness of the limbs (rigidity), slow rhythmic tremors, psychosis, anxiety, depression, and cognitive impairment. Studies indicate that cannabis may enhance PD-induced motor dysfunction, and can improve motor problems such as resting tremors, rigidity, bradykinesia, and posture;
- Alzheimer’s Disease: Alzheimer’s Disease (AD) is characterized by the loss of synapses and the accumulation of plaques composed of a beta-amyloid protein core. Animal studies have shown that compounds that elevate endocannabinoid levels in the brain decrease the toxic effects of beta amyloid peptide. Studies with an AD mouse model have shown that a THC-CBD mix decreased amyloid beta levels and reversed learning impairments;
- Bone diseases:
- Osteoporosis: Osteoblasts (OBs) are those cells which synthesize bone tissue. Activation of CB1 receptors in OBs inhibits the release of norepinephrine, which will suppress the process of bone formation. However, CB2 activation in osteoclasts (OCs) will suppress osteolysis activity, thereby preserving bone tissue. Hence, CB2 provides a molecular target for the diagnosis and treatment of osteoporosis;
- Osteoarthritis: Osteoarthritis is characterized by degeneration of the articular cartilage, and is mediated by proinflammatory cytokines (Xin, et. al., 2022) such as IL-1. Cannabinoids have been shown to prevent IL-1-induced matrix breakdown of collagen and proteoglycan, so that they may play a role in protecting cartilage;
- Bone tumors: The activation of cannabinoid receptors can inhibit tumor cell proliferation, reduce tumor cell invasion, cause tumor regression and prevent tumor metastasis;
- Bone fractures: Cannabinoids have been shown to induce bone formation and strengthen the bridge that connects broken bones. Furthermore, CBD has been shown to stimulate mRNA expression of a particular gene, Plod1, in primary osteoblast cultures to encode an enzyme that catalyzes lysine hydroxylation, which in turn is involved in collagen cross-linking and stabilization. These data show that CBD can improve fracture healing.
- Viral diseases: Cannabinoids demonstrate antiviral potential by blocking of SARS-CoV-2 translation and replication (Bukowska, 2024);
- Cancer: Leinen, et. al, (2023) admit “The endocannabinoid system’s role in cancer is largely unknown and understudied.” However:
- Researchers have found that a disruption in the number of CB1 or CB2 receptors in selected tissues is linked in cancer development and progression. For example, mice models have shown that a reduction in CB1 receptor expression with colorectal carcinoma cells, whereas an elevation in CB1 receptor expression is observed in hepatocarcinoma and Hodgkin’s lymphoma. Research has shown that CBD can induce cancer cell death, particularly in lung cancer cells, and can downregulate vascular endothelial growth factors to decrease cell proliferation;
- Cannabinoids have shown promise in pain management among several groups of patients (Skorzewska and Geca 2024):
- Those in palliative care who have life-limiting illness
- Those experiencing chronic non-cancer pain
- The use of cannabis shows improvement in symptoms such as nausea, vomiting, mood, fatigue, and weight loss;
- In preclinical studies, THC demonstrates significant antitumor effects. For example, Skorzewska and Geca (2024) mention a study involving patients with glioblastoma multiforme (GBM). In this study, three out of nine patients showed clinical and/or radiographic improvement, and two exhibited decreased tumor-cell proliferation on repeat biopsies. Granted, the results of these studies are based on a very limited number of patients, but they point to promising applications.
- In vivo studies have shown anticancer properties by the induction of cell death, mainly by apoptosis (programmed cell death) and cytotoxic autophagy, and the inhibition of cell proliferation. Cannabinoids have been used to treat melanoma and brain glioblastoma. Furthermore, the use of a THC:CBD blend with temozolomide (TMZ) in the treatment of highly invasive brain cancer appear very promising;
IV. Approved cannabis-related drugs
The following table is adapted from Table 3 of Gabarin, et. al. 2023:
| Drug | Active ingredient | Approved use | Other uses |
| Cannabidiol (Epidiolex(R)) | CBD | Rare, severe forms of epilepsy | Anxiety, anti-psychotic effects on schizophrenia, pain, Parkinson’s Disease, cancer, Crohn’s disease |
| Dronabinol (Marinol(R)) | Synthetic cannabinoid | Anorexia associated with weight loss in patients with AIDS; nausea and vomiting associated with cancer chemotherapy | Promotes appetite, anti-emetic, analgesic, treating cannabis addiction, multiple sclerosis |
| Nabilone (CesametTM) | Synthetic cannabinoid, different from Dronabinol | Nausea and vomiting associated with cancer chemotherapy | Fibromyalgia and multiple sclerosis; nightmares in PTSD |
| Rimonabant (Accomplia(R)) | Not a cannabinoid compound, but a CB1 receptor inhibitor | Anti-obesity drug | Diabetes, drug dependence, cancer, atherosclerosis, smoking cessation |
| Nabiximols (Sativex(R)) | THC and CBD | Neuropathic pain, spasticity, overactive bladder, and other symptoms of multiple sclerosis |
V. The use of cannabinoids is not without risk.
The following table is adapted from Table 2 of Johnson et. al. (2025), in which they list the risks and side effects of cannabis use:
| Body System | Potential risks and Side Effects | Notes |
| Central Nervous System | Cognitive impairment, dizziness, sedation, impaired memory, attention deficits, psychosis | Higher THC concentrations increase psychoactive effects |
| Psychiatric | Anxiety, paranoia, depression, cannabis use disorder | Risk likely based on genetic predisposition and on frequency of use |
| Cardiovascular | Tachycardia, orthostatic hypotension | Effect may be more pronounced in older adults |
| Respiratory | Chronic bronchitis, cough, airway inflammation, increased risk of lung cancer if smoked | Vaporized or oral formulations may reduce respiratory risks |
| Gastrointestinal | Nausea, vomiting, Cannabinoid Hyperemesis Syndrome | More common in chronic, high dose use |
| Endocrine and Metabolic | Altered glucose metabolism, appetite stimulation | |
| Reproductive System | Decreased sperm count and mobility, potential impact on ovulation and fetal development | |
| Immune System | Potential suppression of immune response | |
| Fetal Development | Fetal growth restriction, low birth weight, small for gestational age, increased incidence of neurocognitive and neuropsychiatric disorders | Demonstrated in fetuses of mothers who use cannabis during pregnancy |
In a review published in November, 2025, Hsu, et. al., stated that evidence is insufficient for the use of cannabis or cannabinoids for most medical indications, and mention the following observations:
- High-potency cannabis compared with low-potency cannabis use is associated with increased risk of psychotic symptoms (12.4% vs 7.1%) and generalized anxiety disorder (19.1% vs 11.6%);
- A meta-analysis of observational studies reported that 29% of individuals who used cannabis for medical purposes met criteria for cannabis use disorder. Daily inhaled cannabis use compared with nondaily use was associated with an increased risk of coronary heart disease (2.0% vs 0.9%), myocardial infarction (1.7% vs 1.3%), and stroke (2.6% vs 1.0%);
- Evidence from randomized clinical trials does not support the use of cannabis or cannabinoids for most conditions for which it is promoted, such as acute pain and insomnia.
Bukowska, B. (2024). Current and Potential Use of Biologically Active Compounds Derived from Cannabis sativa L. in the Treatment of Selected Diseases. International Journal of Molecular Sciences 25:12738. https://doi.org/10.3390/ijms252312738.
Gabarin, A.; Yarmolinsky, L.; Budovsky, A.; Khalfin, B.; Ben-Shabat, S. (2023). Cannabis as a Source of Approved Drugs: A New Look at an Old Problem. Molecules 28:7686. https://doi.org/10.3390/molecules28237686.
Hsu, M.; Shah, A.; Jordan, A.; Gold, M.S.; Hill, K.P. (2025). Therapeutic Use of Cannabis and Cannabinoids: A Review. JAMA. doi:10.1001/jama.2025.19433. Published online November 26, 2025.
Johnson, B.W.; Strand, N.H.; Raynak, J.C.; Jara, C.; Habtegiorgis, K.; Hand, B.A.; Hong, S.; Maloney, J.A. (2025). Cannabinoids in Chronic Pain Management: A Review of the History, Efficacy, Applications, and Risks. Biomedicines 15:530. https://doi.org/10.3390/biomedicines13030530.
Leinen, Z.J.; Mohan, R.; Premadasa, L.S.; Acharya, A.; Mohan, M.; Byrareddy, S.N. (2023). Therapeutic Potential of Cannabis: A Comprehensive Review of Current and Future Applications. Biomedicines 11:2630. https://doi.org/10.3390/biomedicines11102630 .
Lowe, H.; Toyang, N.; Steele, B.; Bryant, J.; Ngwa, W.; Nedamat, K. (2021). The Current and Potential Application of Medicinal Cannabis Products in Dentistry. Dentistry Journal 9:106. https://doi.org/10.3390/dj9090106.
Martin, K.; Glaser, D.A. (2011). Cosmeceuticals: The New Medicine of Beauty. Missouri Medicine 108(1):60-63.
Prommaban, A.; Kheawfu, K.; Chittasupho, C.; Sirilun, S.; Hemsuwimon, K.; Chaiyana, W. (2022). Phytochemical, Antioxidant, Antihyaluronidase, Antityrosinase, and Antimocribial properties of Nicotiana tabacum. Hindawi Evidence-Based Complementary and Alternative Medicine Volume 2022, Article ID 5761764. https://doi.org/10.1155/2022/576764.
Skorzewska, M.; Geca, K. (2024). The Role of Cannabinoids in Advancing Cancer Treatment: Insights from Evidence-Based Medicine. Current Oncology Reports 26:1334-1348. https://doi.org/10.1007/s11912-024-01589-4.
Stahl, V.; Vasudevan, K. (2020). Comparison of Efficacy of Cannabinoids versus Commercial Oral Care Products in Reducing Bacterial Content from Dental Plaque: A Preliminary Observation. Cureus 2020, 12, e6809.
Xin, Y.; Tang, A.; Pan, S.; Zhang, J. (2022). Components of the Endocannabinoid System and Effects of Cannabinoids Against Bone Diseases: A Mini-Review. Frontiers in Pharmacology 12:793750. doi:10.3389/fphar.2021.793750.
Zou, X.; BK, A.; Abu-Izneid, T.A.; Aziz, A. Devnath, P.; Rauf, A.; Mitra, S.; Bin Emran, T.; Mujawah, A.A.H.; Lorenzo, J.M.; Mubarak, M.S.; Wilairatana, P.; Suleria, H.A.R. (2021). Current advances of functional phytochemicals in Nicotiana plant and related potential value of tobacco processing waste: A review. Biomedicine & Pharmacotherapy 143:112191. https://doi.org/10.1016/j.biopha.2021.112191.


