
I. Coffee
Molecular structure of caffeine. It astounds me that people actually drink coffee for the flavor. WHAT IS THE MATTER WITH THESE PEOPLE?
There is a section in a previous post, https://addictionsandrecoverydotblog.com/2025/03/11/49-it-is-with-a-heavy-heart-that-i-report-to-you-that-the-world-health-organization-recognizes-a-diagnosis-of-caffeine-dependence-syndrome/ , in which I list the benefits of (black) coffee. The crucial infographic from that post is the following:
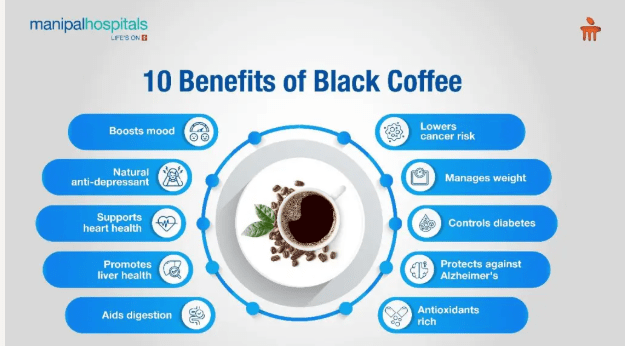
The above is an impressive list of benefits. The benefits that are provided by the consumption of coffee are probably due to the fact that the beverage contains about 2,000 compounds which are known to have antioxidant, antimicrobial, anti-inflammatory, antihypertensive and prebiotic activity. Most of the research has been conducted on caffeine, chlorogenic acids, melanoidins, diterpenes, and trigonelline.
Lopes and Cunha (2024) look at the benefits of coffee intake through the lens of aging, that the consumption of coffee, particularly caffeinated coffee, provides numerous benefits to provide quality of life as people get older.
Lopes and Cunha point out that aging is the major predictor of the development of most chronic debilitating diseases such as stroke, cardiovascular diseases, cancer, Alzheimer’s disease and other dementia, and chronic obstructive pulmonary disease. Furthermore, there is a gradual deterioration of processes that quality of life, including progressive frailty, poorer sleep quality, deterioration of sensory systems, depression and difficulties in decision making. The consensus is that the greatest benefit can be derived from the consumption of 2-3 cups of coffee daily, and here some reasons why:
Boosts mood and is a natural anti-depressant
Healthy older adults habitually drinking coffee tend to report a heightened mood status and improved behavior upon intake of coffee or caffeine. Health older adults also demonstrate increases in psychomotor performance measures of attention, functional performance, manual dexterity, and readiness to invest effort.
Regular and moderate caffeine intake reduces suicide ideation (Park, et. al., 2019). Furthermore, in a pooled analysis of three large-scale US-based cohorts of middle-aged men and women, each additional two cups/day of coffee consumed as was associated with a 25% lower risk of suicide (Lucas, et. al, 2014).
Lowers cancer risk:
There is accumulating evidence to show an inverse association of the intake of moderate doses of coffee with the incidence of some types of cancer, such as:
- Hepatocellular cancer (Bhurwal, et. al., 2020);
- Melanoma (Micek, et. al., 2018); and
- Colorectal cancer (Wang, et. al., 2020)
Controls diabetes:
Coffee intake exerts beneficial effects in individuals with type 2 diabetes (Carlstrom and Larsson, 2018).
Protects against Alzheimer’s Disease
Zhang, et. al. (2026) describe a prospective cohort study of 131,821 individuals from 2 cohorts with up to 43 years of follow-up. One cohort consisted of female participants from the Nurses’ Health Study (NHS; n-86,606 with data from 1980-2023). The other cohort consisted of male participants from the Health Professionals Follow-up Study (HPFS; n=45,215 with data from 1986-2023. Of these individuals, 11,033 dementia cases were documented, although the abstract does not specify Alzheimer’s Disease. After adjusting for potential confounders and pooling results across cohorts, higher caffeinated coffee intake was significantly associated with lower dementia risk (141 vs 330 cases per 100,000 person-years) and lower prevalence of subjective cognitive decline. Higher intake of tea showed similar associations with these cognitive outcomes, whereas decaffeinated coffee intake was NOT associated with lower dementia risk or better cognitive performance. The most pronounced associated differences were observed with intake of approximately 2 to 3 cups per day of caffeinated coffee or 1 to 2 cups per day of tea.
Supports heart health
An article published in 2025 shows that the consumption of a modest amount of caffeinated coffee per day reduces the likelihood of atrial fibrillation episodes (Wong, et. al., 2025).
What is atrial defibrillation?
The following is a description of atrial defibrillation from MedlinePlus, https://medlineplus.gov/atrialfibrillation.html#:~:text=Atrial%20fibrillation%2C%20also%20known%20as,Aging:
Atrial fibrillation, also known as AFib or AF, is one of the most common types of arrhythmias. Arrhythmias are problems with the rate or rhythm of your heartbeat. They can cause your heart to beat too slowly, too fast, or in an irregular way.
Here is an image showing the difference between a normal electrocardiogram and another showing atrial fibrillation:
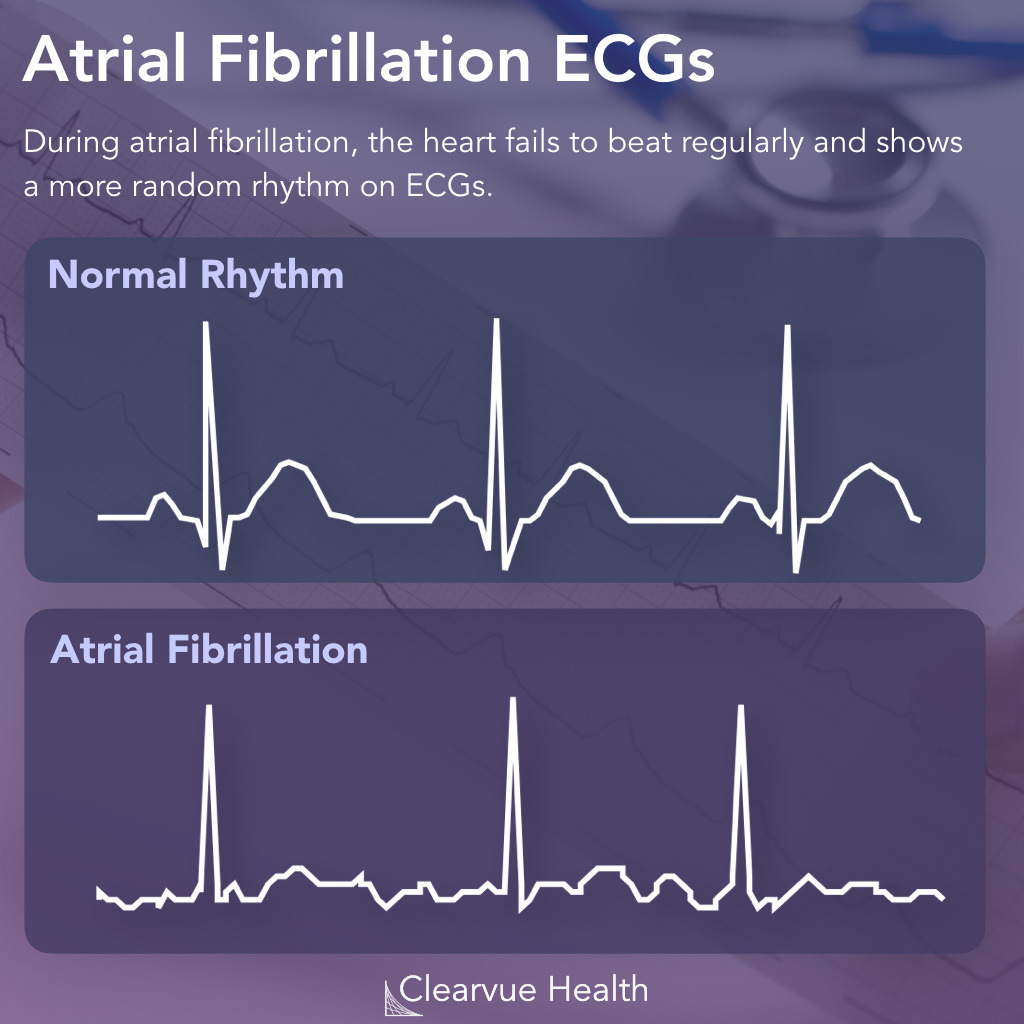
When this happens, the lower chambers do not fill completely or pump enough blood to your lungs and body. This can cause symptoms such as dizziness, fatigue, and a pounding heartbeat. AFib may happen in brief episodes, or it may be a permanent condition. It’s very important to treat it, since AFib can put you at risk for stroke and other heart conditions.
AFib is most often caused by changes to the heart’s tissue or the electrical signaling that helps the heartbeat. These changes can happen due to different conditions and factors, such as high blood pressure, coronary artery disease, congenital heart defects, infections, and aging. Sometimes the cause is unknown.
The symptoms of AFib can include:
- Extreme fatigue, which is the most common symptom
- Heart palpitations (the feeling that your heart is skipping a beat, fluttering, pounding, or beating too hard or too fast)
- Trouble breathing, especially when lying down or when exercising
- Chest pain
- Dizziness or fainting
- Low blood pressure
If AFib is not treated, it can lead to serious health problems (complications) such as:
- Stroke
- Heart failure
- Blood clots
- Sudden cardiac arrest (SCA)
- Cognitive impairment and dementia
What’s the evidence favoring the consumption of coffee to avoid episodes of atrial defibrillation?
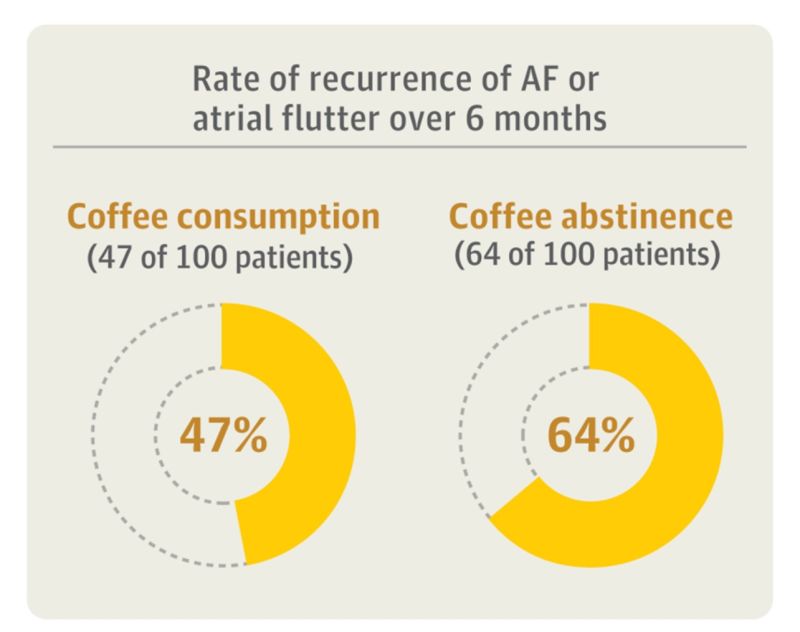
Wong, et. al. (2025) recruited 200 participants who had a history of coffee drinking and persistent atrial fibrillation (or atrial flutter with a history of atrial fibrillation) after successful cardioversion. The average age was 69 years, 71% of whom were male and 29% female. These participants were divided into two groups, one of which consumed at least one cup of caffeinated coffee daily, and the other abstained from all coffee and caffeine.
The results show that those individuals who consumed caffeinated coffee daily had a reduced incidence of atrial fibrillation episodes:
In an article appearing in the 23 January 2026 issue of the Huffington Post ( https://www.huffingtonpost.co.uk/entry/coffee-ageing-longevity_uk_69734557e4b0283a0977445d?ncid=APPLENEWS00001 ), Amy Glover refers to a 2024 paper (Lopes and Cunha, 2024) which suggests that coffee could reduce your risk of all-cause mortality, ageing-related conditions like stroke, help your stress adaptation mechanisms, and even protect your body as it ages.
These authors looked at over 50 existing coffee and ageing studies from around the drink to determine how coffee seemed to affect the ageing process, the risk for diseases like cancer, stroke, and heart disease, and its effects on sleep, cognition, and depression.
In other words, Juan Valdez would approve. (https://flavorsofbogota.com/who-is-juan-valdez/)
II. Dark chocolate
The Kuna Indians of the San Blas islands of Panama provide a clue as to just how effective cocoa is to promote health:

Image from https://www.flickr.com/photos/kramirez/116664720
Image from https://sanblas-islands.com/getting-there/
The Kuna Indians consume an average of three 10-ounce cups of cocoa beverage daily, ingesting approximately 1880 mg of procyanidins. Recent on these people shows that the prevalence of hypertension among them is very low (2.2%) and blood pressure (BP) does not increase with age. Furthermore, the population also experiences lower rates of diabetes mellitis, myocardial infarction, stroke, and cancer than mainland Panamanians (Katz, Doughty, and Ali, 2011).
When, however, Kuna migrate to urban areas on the mainland, the prevalence of hypertension is higher (10.7%) and reaches 45% among those over age 60.
Components of cocoa
Cocoa is the dried and fully fermented fatty seed of the fruit of the cocoa tree, Theobroma cacao. Cocoa liquor is the paste made from ground, roasted, shelled, and fermented coca beans, called nibs. These nibs contain both nonfat cocoa solids and cocoa butter. Cocoa liquor is the indicator for “percent cacao” on food packaging. Cocoa powder is produced by removing some of the cocoa butter from the liquor, while chocolate is a solid food made by combining cocoa butter and sugar. The proportion of cocoa liquor in the final product determines how dark the chocolate is.
While cocoa cutter contains significant amounts of fatty acids, it is the nonfat cocoa solids which contain vitamins, minerals, fiber and polyphenolic antioxidants.
- Lipids: The oil in cacao, referred to as cocoa butter, is a mixture of monounsaturated and saturated fatty acids. Typically, saturated fatty acids are associated with an increased risk of coronary heart disease, since saturated fatty acids elevate total cholesterol. However, cocoa butter is rich in steric acid, which is unusual in that it does NOT elevate serum lipid levels to the same degree that other fatty acids do;
- Fiber: The majority of fiber in cocoa is insoluble, which has been associated with reduced risk of type 2 diabetes;
- Minerals: Cocoa beans contain several minerals for vascular function, including magnesium, copper, potassium and calcium, all of which reduce risk of hypertension and atherosclerosis.
- Magnesium is also a cofactor in protein synthesis, muscle relaxation and energy production;
- Copper is a cofactor for enzymes required for a variety of processes, including iron transport, glucose metabolism, infant growth, and brain development;
- Dietary potassium may protect against hypertension caused by excess sodium intake;
- Polyphenols: Cocoa powder contains up to 50 mg of polyphenols per gram. “Single servings of cocoa and cocoa products contain more phenolic antioxidants than most foods, and more procyanidins than the average amount consumed by Americans per day (Katz, Doughty, and Ali, 2011).”
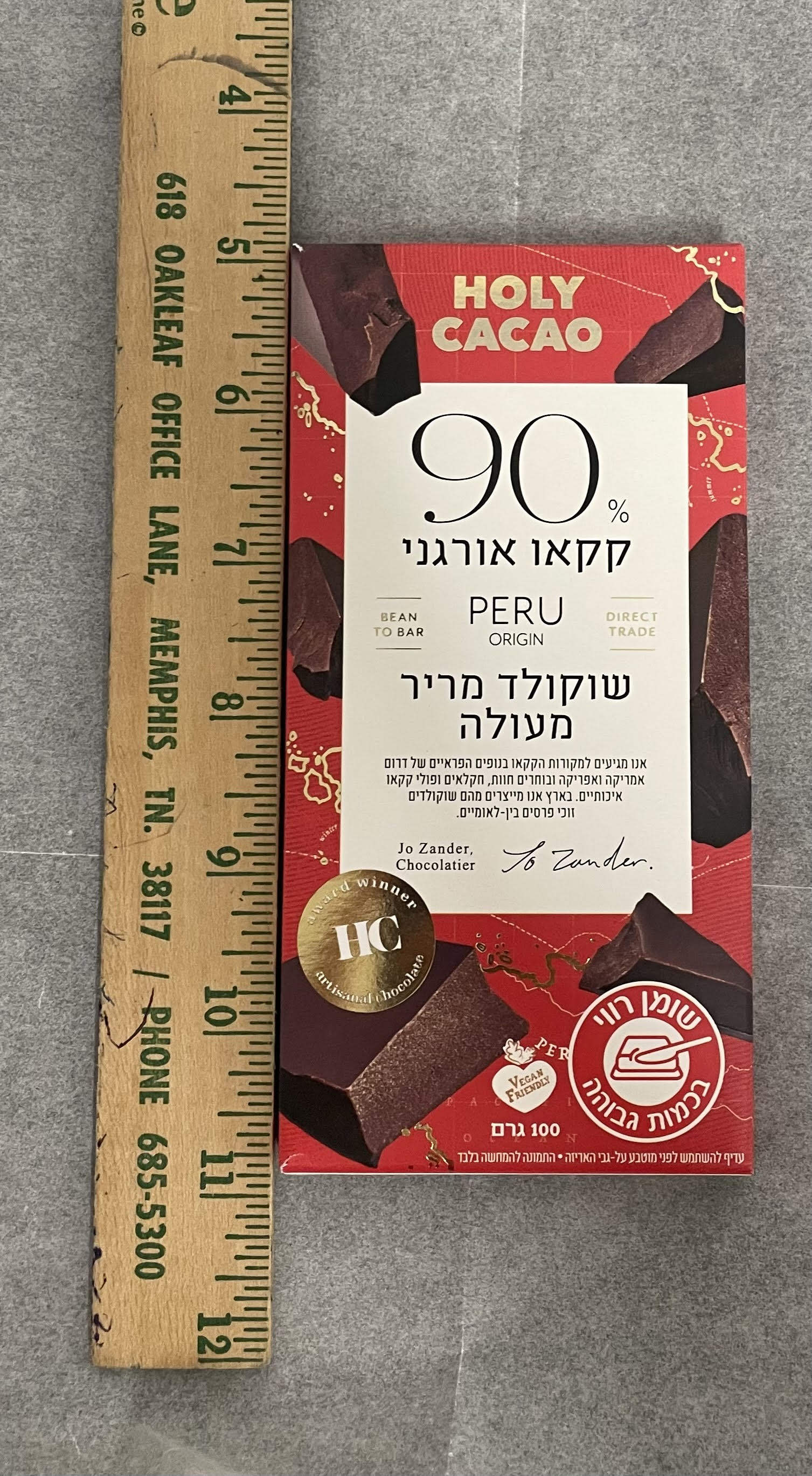
Before we go any further, I think it would be worthwhile to establish a standard when discussing the benefits of ingesting cocoa or chocolate as a function of the amount consumed. The following photographs, taken by yours truly, show what 21 grams of dark chocolate looks like (on the left), and what a 100 gram bar looks like (on the right):

There is considerable research devoted to the antioxidant properties of cocoa and their beneficial effects on various organ systems and processes. That is the topic of the next section:
The principal antioxidants in cocoa
The principal family of antioxidants are called flavonoids, and they include catechin, epicatechin, and procyanidins. Notice the similarities in their structures.
Structure of Catechin:
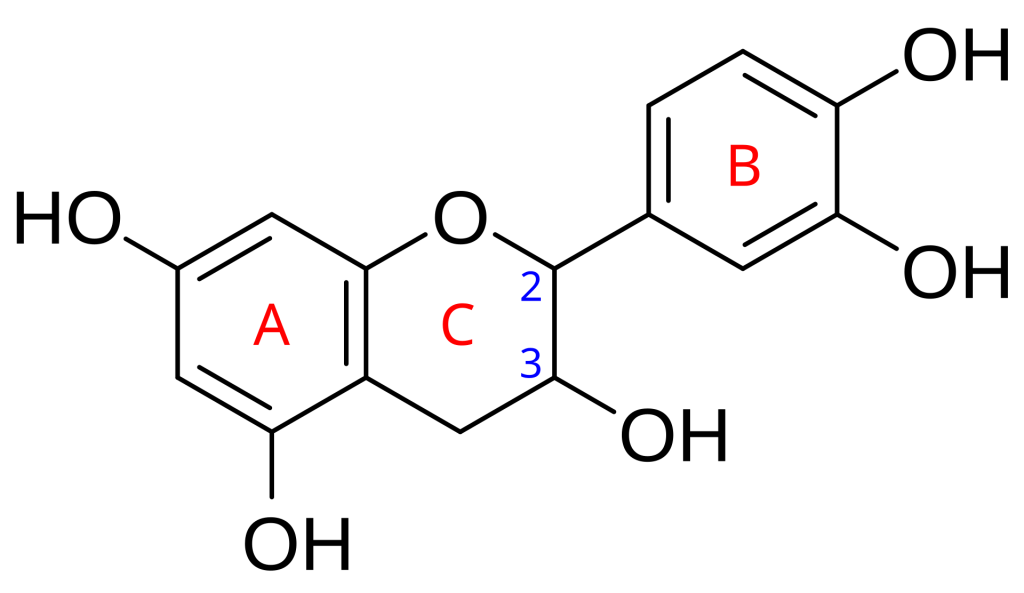
User:Innerstream, Public domain, via Wikimedia Commons
Structure of Epicatechin:
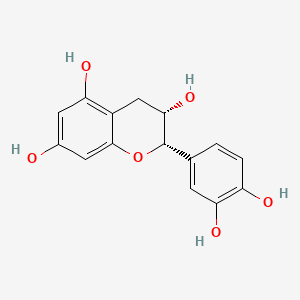
Image from https://pubchem.ncbi.nlm.nih.gov/compound/ent-Epicatechin#section=2D-Structure
Structure of Procyanidins:
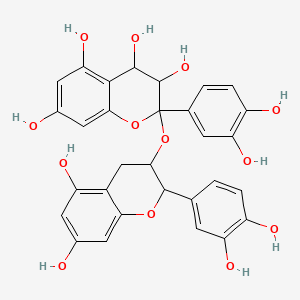
Image from https://pubchem.ncbi.nlm.nih.gov/compound/Procyanidin
The following is a list of statements describing the benefits of cocoa/chocolate, with each statement followed by supporting references:
The consumption of cocoa reduces the risk of all-cause mortality and cardiac death, and prevents the formation of atherosclerotic plaques.
For example, in 2006, Buijsse, et. al. published the results of a cohort study of 470 Dutch men which showed clear benefits to ingesting cocoa. The men in this study were free of cardiovascular disease and of diabetes, and were part of the Zutphen Elderly Study cohort. Researchers found that systolic and diastolic blood pressures (BPs) were inversely associated with cocoa intake after adjustment for a wide of possible confounders. Cocoa consumption was associated with significantly lower cardiovascular and all-cause mortality. Furthermore, those in the highest tertile of cocoa intake compared with those in the lowest tertile had 50% lower rates of all-cause mortality and cardiovascular disease. Individuals in the highest tertile consumed more than 2.30 grams if cocoa daily, whereas those in the lowest tertile consumed less than .36 grams/day (Buijsse, Feskens, Kok, and Kromhout, 2006.)
Similar results were found in a study by Janszky, et. al. (2009). In this case, the sample population included nondiabetic patients hospitalized with a first myocardial infarction. After a mean 8.6 years of follow-up, patients who reported eating chocolate twice or more per week were 66% less likely to suffer a cardiac death compared to those who reported never eating chocolate.
The consumption of chocolate also has a beneficial effect on preventing the formation of atherosclerotic plaques. A study of 2217 participants in the HNLBI Family Heart Study showed an inverse relationship between chocolate consumption and calcified atherosclerotic plaque in the coronary arteries. Individuals who consumed chocolate two or more times per week were 32% less likely to have prevalent coronary calcification compared with those who never ate chocolate (Djousse, et. al., 2011).
The consumption of “chocolate snack pieces” reduces the risk of developing diabetes.
In a Japanese study, the risk of being found to have diabetes was 35% among men who consumed “chocolate snack pieces” once per week or more compared with those who never or almost never ate chocolate (Oba, et. al., 2010). While this finding was statistically significant among men, a similar finding among women was not statistically significant.
The concentration of serum C-reactive protein (CRP), a measure of inflammation, is reduced among men and women who consume dark chocolate.
According to https://my.clevelandclinic.org/health/diagnostics/23056-c-reactive-protein-crp-test, C-reactive protein is released by the liver into the bloodstream in response to inflammation. “Healthcare providers use this test to help diagnose and monitor several different causes of inflammation, such as infections and certain autoimmune conditions”, including the following:
- “Severe bacterial infections, such as sepsis;
- Fungal infections;
- Osteomyelitis (infection of your bone);
- Inflammatory bowel disease (IBD);
- Some forms of arthritis;
- Autoimmune diseases, such as rheumatoid arthritis or lupus (systemic lupus erythematosus);
- Pelvic inflammatory disease (PID).”
Having said that, in a study of Italian men and women, individuals consuming a 20-gram serving of dark chocolate daily had the lowest CRP concentrations (di Giuseppe, et. al., 2008).
Evidence shows that the consumption of chocolate improves mood and relieves depression.
In 2009, Strandberg, et. al. found a relationship between psychological health and chocolate preference in elderly men preferring chocolate reported feeling less lonely and depressed and happier than men preferring other types of candy.
*******************************************************
What about craving?
A considerable amount of research on cocoa’s effect on psychological variables has focused on the phenomenon of craving, probably because so many people crave it. Women tend to crave chocolate more than men, particularly during the perimenstrual period (Bruinsma and Taren, 1999; Rozin, Levine and Stoess, 1991; Zellner, et. al., 2004.) It appears, however, that it is not the bioactive compounds in the cocoa itself, but rather it is the particular taste and mouth-feel of solid chocolate products which satisfy chocolate cravings.
Perhaps, therefore, it is no coincidence that an icon for St. Valentine’s Day is a heart-shaped box of chocolates that the male of the species is expected to give to the female. In the animal world, when a male brings a food gift to a female, it is because the male has made considerable progress in terms of the courtship ritual, and now the male expects something from the female in return for his gift of food. (I guess animals dispense with the theatre part of the ritual.)

Image from https://www.lakechamplainchocolates.com/grand-valentine-chocolate-heart/
This brought up the question as to whether females and males differ in their preference for white chocolate, milk chocolate, and dark chocolate.
One of the laboratory exercises my students conducted in my Biology of Addiction class was designed to address that particular issue. We gave, under the direction of Marian Hughes, manager of the local Godiva Chocolatier and later Dinstuhl’s Chocolates, each participating university student three wafers: White chocolate, Milk Chocolate, and Dark chocolate. For each wafer, each participant was to smell the fragrance, hear the sound of the wafer as it was broken, and then take tiny nibbles from the wafer and let each nibble melt in his/her mouth. Afterward, each participant filled out a survey to indicate which flavor was her/his favorite, and here the results:
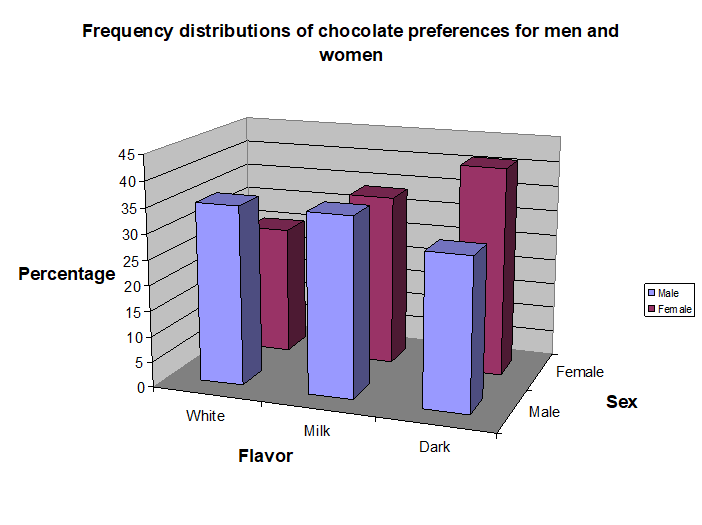
While the preference distribution for males was more evenly distributed among the three flavors, the female participants tended towards the milk and dark chocolates.
As you may guess, this was one of the favorite laboratory exercises of the semester, as evidenced by the facial expressions of the participants. IMHO, these students are in ecstasy:


Which finally brings me to the following observations, which I will NOT dispute:
Some reasons why women consider chocolate more reliable than men (From http://menjokes.torch.net.pl/choco.html):
•1. Chocolate satisfies every time.
•2. Chocolate doesn’t care how many pieces you’ve eaten before.
•3. Chocolate never leaves a bad taste in your mouth.
•4. You always know if someone else has eaten any of your chocolate.
•5. One taste and you can’t help but want more.
•6. If it gets soft, a few seconds in the refrigerator will make it hard again.
•8. Size really doesn’t matter.
P.S.: Ooh, yum!

(Image AI generated.)
Buijsse B, Feskens EJ, Kok FJ, and Kromhout D. (2006). Cocoa intake, blood pressure, and cardiovascular mortality: the Zutphen elderly study. Arch Intern Med 166: 411–417.
Bhurwal, A., Rattan, P., Yoshitake, S., Pioppo, L., Reja, D., Dellatore, P., Rustgi, V., 2020. Inverse association of coffee with liver cancer development: an updated systematic review and meta-analysis. J. Gastrointestin Liver Dis. 29(3):421-428. https://doi.org/10.15403/jgld-805.
Bruinsma K and Taren DL. (1999). Chocolate: food or drug? J Am
Diet Assoc 99: 1249–1256.
Carlstrom, M., Larsson, S.C. (2018). Coffee consumption and reduced risk of developing type 2 diabetes: a systematic review with meta-analysis. Nutr. Rev. 76 (6), 395–417.
https://doi.org/10.1093/nutrit/nuy014
di Giuseppe R, Di Castelnuovo A, Centritto F, Zito F, De
Curtis A, Costanzo S, Vohnout B, Sieri S, Krogh V, Donati
MB, de Gaetano G, and Iacoviello L. (2008). Regular consumption of dark chocolate is associated with low serum concentrations of C-reactive protein in a healthy Italian population. J Nutr 138: 1939–1945.
Djousse L, Hopkins PN, Arnett DK, Pankow JS, Borecki I,
North KE, and Curtis Ellison R. (2011). Chocolate consumption is inversely associated with calcified atherosclerotic plaque in
the coronary arteries: The NHLBI Family Heart Study. Clin
Nutr 30: 38–43.
Janszky I, Mukamal KJ, Ljung R, Ahnve S, Ahlbom A, and
Hallqvist J. (2009). Chocolate consumption and mortality following a first acute myocardial infarction: the Stockholm Heart
Epidemiology Program. J Intern Med 266: 248–257.
Katz, D.L.; Doughty, K.; Ali, A. (2011). Cocoa and Chocolate in Human Health and Disease. Antioxidants & Redox Signaling 15(10):2779-2811. https://doi.org/10.1089/ars.2010.3697.
Lopes, C.R.; Cunha, R.A. (2024). Impact of coffee intake on human aging: Epidemiology and cellular mechanisms. Ageing Research Reviews 102: 102581. https://doi.org/10.1016/j.arr.2024.102581.
Park, H.; Suh, B.S.; Lee, K. (2019). Relationship between daily coffee intake and suicidal ideation. Journal of Affective Disorders, 256:468-472. https://doi.org/10.1016/j.jad.2019.06.023
Lucas, M., O’Reilly, E.J., Pan, A., Mirzaei, F., Willett, W.C., Okereke, O.I., Ascherio, A. (2014). Coffee, caffeine, and risk of completed suicide: results from three prospective
cohorts of American adults. World J. Biol. Psychiatry 15 (5), 377–386. https://doi.org/10.3109/15622975.2013.795243.
Micek, A., Godos, J., Lafranconi, A., Marranzano, M., Pajak, A. (2018). Caffeinated and decaffeinated coffee consumption and melanoma risk: a dose-response meta-analysis of prospective cohort studies. Int. J. Food Sci. Nutr. 69 (4), 417–426. https://doi.org/10.1080/09637486.2017.1373752 .
Oba S, Nagata C, Nakamura K, Fujii K, Kawachi T, Takatsuka
N, and Shimizu H. (2010). Consumption of coffee, green
tea, oolong tea, black tea, chocolate snacks and the caffeine
content in relation to risk of diabetes in Japanese men and
women. Br J Nutr 103: 453–459.
Rozin P, Levine E, and Stoess C. (1991). Chocolate craving and
liking. Appetite 17: 199–212.
Strandberg TE, Strandberg AY, Pitkala K, Salomaa VV, Tilvis
RS, and Miettinen TA. (2008). Chocolate, well-being and health
among elderly men. Eur J Clin Nutr 62: 247–253.
Wang, Y., Chen, J., Zhao, R., Xia, L., Cui, Y.P., Rao, Z.Y., Zhou, Y., Wu, X.T., 2020. Doseresponse meta-analysis of coffee consumption and risk of colorectal adenoma. Eur. J.
Clin. Nutr. 74 (2), 297–306. https://doi.org/10.1038/s41430-019-0467-0.
Wong, C.X.; Cheung, C.C.; Montenegro, G.; Oo, H.H.; Pena, I.J.; Tang, J.J.; Tu, S.J.; Wall, G.; Dewland, T.A.; Moss, J.D.; Gerstenfeld, E.P.; Tseng, Z.H.; Hsia, H.H.; Lee, R.J.; Olgin, J.E.; Vadentham, V.; Scheinman, M.M.; Lee, C.; Sanders, P.; Marcus, G.M. (2025). Caffeinated Coffee Consumption or Abstinence to Reduce Atrial Fibrillation: The DECAF Randomized Clinical Trial. JAMA. doi:10.1001/jama.2025.21056
Zellner DA, Garriga-Trillo A, Centeno S, and Wadsworth
E. (2004). Chocolate craving and the menstrual cycle. Appetite 42:
119–21.
P.P.S.:


