
(Illustration from https://cancercontrol.cancer.gov/sites/default/files/2020-06/chapter_3_smokelesstobaccoandpublichealth.pdf)
What is smokeless tobacco?
Smokeless tobacco is any form of shredded or crushed tobacco which can be placed in the mouth, usually between the gums and the cheek of lips, or can be sniffed or snorted up the nose.
In all cases, smokeless tobacco products contain nicotine, an addictive stimulant drug. When it enters the body, either through the nasal mucosa or the mouth, it will cause the adrenal glands to release adrenaline (epinephrine), which in turn, will cause an increase in heart rate.
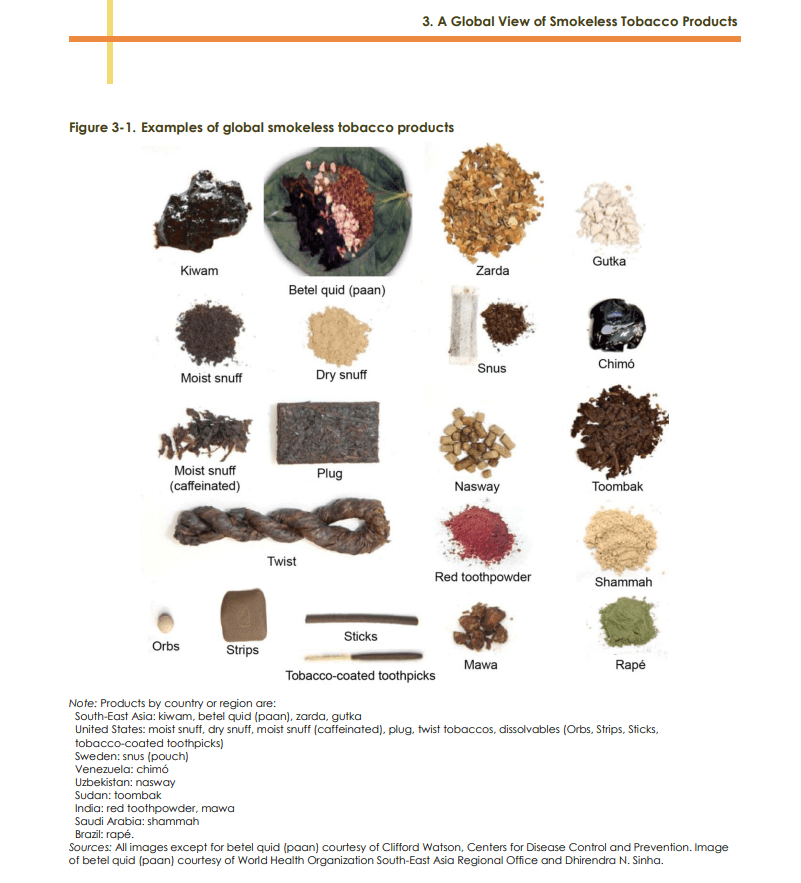
Types of smokeless tobacco
The three main types of smokeless tobacco (perhaps in the US and Europe) include the following:
- Chewing tobacco
- Snuff
- Snus
In Table 1, Hajat, et. al. (2021) list an additional 25 types of smokeless tobacco, mainly of which are used only in the Region of the Americas (AMR) or in the South-East Asian Region (SEAR).
Chewing tobacco

Chewing tobacco is large, dried (cured), dark brown tobacco leaves — it looks like tea leaves. It may be a loose pile of leaves, or it may look like a dense brick (plug) or braid (twist). People typically pinch the leaves between their thumbs and pointer fingers and place it between their gums and cheeks or lips. Or they may cut or bite a piece off the plug or chew and place it in the same area. Most people spit out tobacco juices when they use smokeless tobacco orally. But some people swallow some of it.
Snuff

Illustration extracted from https://dralun.wordpress.com/2014/09/15/the-great-georgian-snuff-debate/
Snuff is finely crushed tobacco. It can either be moist (dip) or dry, and manufacturers typically add artificial flavors, like mint or fruit, and other additives to it.

Image By Hellahulla – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=10995010
People typically pinch moist snuff between their thumbs and fingers and pack it between their gums and cheeks or lips. But it may also come in tiny pouches that resemble tea bags. Dry snuff typically enters your body by snorting it up your nose.
(Ed. note:) In my humble opinion, in order to properly consume snuff, you MUST dress in the attire appropriate for Mozart and wear a white wig. Any other manner would be considered grossly undignified:

Snus

In 2017, Joe Schwarcz stated the following about snus:
Snus, pronounced snoos, is a smokeless form of tobacco which is produced and used essentially only in Norway and Sweden. Snus is typically placed under the upper lip, either as loose tobacco, lössnus or in prepackaged small bags, portionsnus. It is kept in place for an average of 20 minutes delivering a steady stream of nicotine. Unlike the form of chewing tobacco used in North America, snus does not require spitting. It also differs from regular tobacco in that it is steam cured rather than flue cured. This results in lowers levels of carcinogens such as nitrosamines. On the other hand, snus contains higher levels of nicotine.
The health risks are similar
In a previous blogpost, https://addictionsandrecoverydotblog.com/2024/01/07/16-nicotine-iii-the-dreadful-company-that-nicotine-keeps-chemical-components-of-cigarette-smoke-and-their-hazards/, we looked at the dreadful company which nicotine keeps, in the form of carcinogenic and mutagenic compounds that are found in tobacco leaves or are generated by their pyrolysis.
The following infographic, extracted from https://www.verywellhealth.com/snus-health-risks-5089177 and referencing only snus, can be applied to snuff and chewing tobacco:
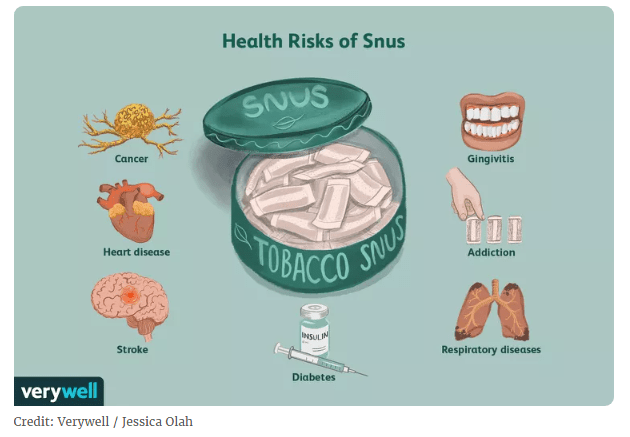
The culprit for some of the risks shown in the infographic shown above is nicotine:
Addiction:
Nicotine is the compound which induces addiction. Addiction to nicotine is so tenacious that approximately 80% of smokers who attempt to quit on their own relapse within the first month of abstinence, and only about 3% remain abstinent at six months (Benowitz, 2009).
The rewarding aspect of nicotine can be explained by its mode of action. Nicotine readily crosses the blood-brain barrier, binds to nicotinic cholinergic receptors (nAChRs), which, in turn, stimulates the release of dopamine in the reward circuitry of the brain.
After nicotine has exerted its effects on the brain, it is readily metabolized, thus inducing unpleasant withdrawal symptoms. The negative emotional state will include anxiety and the perception of increased stress. The negative emotional state is either avoided or reduced with the continued use of nicotine products.
So nicotine from tobacco induces stimulation and pleasure, and reduces stress and anxiety. The use of nicotine may also improve concentration, reaction time, and performance of certain tasks. However, when a person stops smoking, nicotine withdrawal symptoms emerge, and these may include irritability, depressed mood, restlessness, anxiety, problems getting along with friends and family, difficulty concentrating, increased hunger and eating, insomnia, and craving for tobacco (Benowitz, 2009).
Diabetes:
Carlsson, et. al. (2017) compared the hazard ratios of 54,531 Swedish men who never used snus with those who did. Compared to never users, the Hazard Ratio (HR) of type 2 diabetes was 1.15 in current users of snus, suggesting that snus users were at increased risk. In fact, for individuals 5-6 boxes per week, the HR was 1.42, and for those consuming >= 7 boxes, the HR was 1.68. Each additional box of snus consumed per week produced an HR of 1.08.
They suggest that nicotine is responsible for the increase in risk, because nicotine can inhibit insulin sensitivity, thereby promoting abdominal obesity and subsequently insulin resistance.
Cancer:
I. Nicotine’s contribution
Nicotine itself is not a carcinogen, but it may be a tumor promoter (Benowitz, 2009). In Benowitz’s article, he states that in animal studies, nicotine has been shown to inhibit apoptosis, resulting in impaired killing of cancer cells. Furthermore, nicotine promotes angiogenesis, i.e. the formation and development of blood vessels, an effect which could promote tumor invasion and metastasis.
II. And then there are the chemicals in the tobacco leaves themselves.
Table 3.2 in Smokeless Tobacco and Public Health: A Global Perspective, GST Report, https://cancercontrol.cancer.gov/sites/default/files/2020-06/chapter_3_smokelesstobaccoandpublichealth.pdf, contains a LONG list of carcinogens found in smokeless tobacco. The following partial list is extracted from that table:
- Tobacco-specific nitrosamines
- N-Nitrosodimethylamine (NDMA)
- N-Nitrosopyrrolidine (NPYR)
- N-Nitrosopiperidine (NPIP)
- Volatile aldehydes
- Formaldehyde (yes, that compound that gives the fetal pigs you dissected that distinctive, uh, fragrance.)
- Acetaldehyde
- Afltatoxin
- Polycyclic aromatic hydrocarbons
- Benzo[a]pyrene (BaP)
- Benz[a]anthracene (BaA)
- Naphthalene (NAP)
Heart Disease:
In January 2025, the American Heart Association released a policy statement regarding the impact of smokeless oral nicotine products on cardiovascular disease (AHA, 2025). Recent studies have yielded mixed results. For example, one cohort study found that snus use was associated with increased hospitalization for heart failure, including nonischemic heart failure, but another large Swedish population-based cohort study found no association with MI, heart failure, atrial fibrillation, aortic valve stenosis, abdominal aortic aneurysm or stroke, but did find an increased risk of stroke in those who used snus and who never smoked. Similarly, a recent US cohort study found that smokeless tobacco use increased the risk of incident peripheral arterial disease, but a large Swedish cohort study found no such association.
However, pooled analyses of prospective cohort studies in Sweden have confirmed an increased short-term risk of mortality resulting from myocardial infarction (MI, AKA heart attack) and stroke, but no increased risk of acute MI or stroke.
Gingivitis:
According to the Mayo Clinic (https://www.mayoclinic.org/diseases-conditions/gingivitis/symptoms-causes/syc-20354453#:), gingivitis is “a common and mild form of gum disease, also called periodontal disease. It causes irritation, redness, swelling and bleeding of your gingiva, which is the part of your gum around the base of your teeth…Gingivitis does not cause bone loss. But left untreated, it can lead to a much more serious gum disease, called periodontitis, and tooth loss.”
Yadadi, et. al. (2024) examined the prevalence of smokeless tobacco consumption and its effects on gingival and periodontal health among 120 male and 51 female eligible adults who reported to the University Dental Hospital in Sharjah, UAE. between December 2022 and March 2023. Participants’ gingival status and periodontal condition based on Plaque Index (PI) scores, Gingival Recession (GR) scores, Pocket Probing scores (PPD), and Clinical Attachment Level (CAL). (Ed. note: The last is a measured distance from a fixed point on the tooth, usually the cementoenamel junction to the base of the periodontal pocket, which represents how much of the tooth’s supporting attachment has been lost due to periodontal disease.)
They found that the differences in CAL and Gingival recession were significant, while the others were not. They conclude that smokeless tobacco (SLT) usage is substantially linked to a higher risk of periodontal and gingival disease, including periodontitis and gingivitis in adults.
Granted, this study involved a relatively small sample size, but these conclusions are supported by a study conducted by Fisher, et. al., (2005). The results of this population-based study 12,932 adults participating in the Third National Health and Nutrition Examination Survey showed that all adults and never-smokers who currently used smokeless tobacco were twice as likely to have severe active periodontal disease at any site, simultaneously adjusted for smoking, age, race, gender, diabetes, and having a dental visit in the past year.
Respiratory disease:
According to study conducted by Gudnadottir, et. al. (2017), snus use is associated with a higher prevalence of asthma, respiratory symptoms and snoring. The findings of this study are based on the postal questionnaires completed by 26,694 participants aged 16 to 75 years living in Sweden. The questionnaire included questions on tobacco use, asthma, respiratory problems and sleeping problems.
The following table, based on the data presented in Table 3, show a clear, consistent, and significant association between snus and respiratory health and sleep-related symptoms:
| Condition | Never smoked: Tobacco free (n=14914) | Snus users | p Value |
| Asthma | 6.9 | 10.1 | <.001 |
| Chronic bronchitis | 9.0 | 12.5 | <.001 |
| Allergic rhinitis | 24.7 | 28.0 | .012 |
| Sleeping problems: (DIS) (Difficulty inducing sleep) | 11.1 | 16.5 | <.001 |
| Sleeping problems: DMS (Difficulty maintaining sleep) | 25.3 | 15.8 | <.001 |
| Sleeping problems: EDS (Excessive daytime sleepiness) | 28.7 | 29.8 | <.001 |
Smokeless tobacco shows some protection against developing Parkinson’s disease.(!)
I. To answer the question, “what is Parkinson’s Disease?”
The following information is extracted from a website maintained by the Mayo Clinic at https://www.mayoclinic.org/diseases-conditions/parkinsons-disease/symptoms-causes/syc-20376055:
Parkinson’s disease is a movement disorder of the nervous system that worsens over time. The nervous system is a network of nerve cells that controls many parts of the body, including movement.
Symptoms start slowly. The first symptom may be a barely noticeable tremor in just one hand or sometimes a foot or the jaw. Tremor is common in Parkinson’s disease. But the disorder also may cause stiffness, slowing of movement and trouble with balance that raises the risk of falls.
Parkinson’s symptoms may include:
- Tremor. This rhythmic shaking usually begins in the hands or fingers. Sometimes tremor begins in the foot or jaw. You may rub your thumb and forefinger back and forth. This is known as a pill-rolling tremor. Your hand may tremble when it’s at rest or when you’re under stress. You may notice that you shake less when you’re doing some sort of task or moving around.
- Slowed movement, also called bradykinesia. Parkinson’s disease may slow your movement, making simple tasks more difficult. It may be hard to get out of a chair, shower or get dressed. You may have less expression in your face. It may be hard to blink.
- Rigid muscles. You may have stiff muscles in any part of your body. Your muscles may feel tense and painful, and your arm movements may be short and jerky.
- Poor posture and balance. Your posture may become stooped. You may fall or have balance problems.
- Loss of automatic movements. You may be less able to make certain movements that you typically do without thinking, including blinking, smiling or swinging your arms when you walk.
- Speech changes. You may speak softly or quickly, slur, or hesitate before talking. Your speech may be flat or monotone, without typical speech patterns.
- Writing changes. You may have trouble writing, and your writing may appear cramped and small.
- Nonmotor symptoms. These may include depression, anxiety, constipation and sleep problems. They also may include acting out dreams, needing to urinate often, trouble smelling, problems with thinking and memory, and feeling very tired.
Causes
In Parkinson’s disease, nerve cells in the brain called neurons slowly break down or die. Many Parkinson’s disease symptoms are caused by a loss of neurons that produce a chemical messenger in the brain. This messenger is called dopamine.
Decreased dopamine leads to irregular brain activity. This causes movement problems and other symptoms of Parkinson’s disease. People with Parkinson’s disease also lose a chemical messenger called norepinephrine that controls many body functions, such as blood pressure.
The cause of Parkinson’s disease is unknown, but several factors seem to play a role, including:
- Genes. Specific genetic changes are linked to Parkinson’s disease. But these are rare unless many family members have had Parkinson’s disease.
- Environmental factors. Exposure to certain toxins or other environmental factors may increase the risk of later Parkinson’s disease. One example is MPTP, a substance that can be found in illegal drugs and is sometimes sold illegally as “synthetic heroin.” Other examples include pesticides and well water used for drinking. But no environmental factor has proved to be a cause.
A video regarding Parkinson’s Disease:
II. How smokeless tobacco may have a neuroprotective effect, with respect to Parkinson’s Disease.
Hajat, et. al., (2021) refer to an earlier study, (Yang, et. al., 2017) involving a study of 348,601 Swedish men to determine whether snus, like cigarette smoking, confer a lower risk of Parkinson’s disease. In their 2017 study, Yang, et. al. found that among men who never smoked, ever-snus users had about 60% lower Parkinson’s disease risk compared with never-snus users. The inverse association between snus use and Parkinson’s disease risk was more pronounced in current (pooled HR 0.38, 95% CI 0.23-0.63), moderate-heavy amount (pooled HR 0.41, 95% CI 0.19-0.90) and long-term snus users (pooled HR 0.44, 95% CI 0.24-0.83).
(Ed. note: I don’t think there is a physician on earth who will advise a patient, “I think you should start using smokeless tobacco.” If, however, the person is smoking tobacco, then using smokeless tobacco may be the only Plan B available.)
Himmelfarb, C.R.D.; Benowitz, N.L.; Blank, M.D.; Bhatnagar, A.; Chase, P.J.; Davis, E.M.; Fetterman, J.L.; Keller-Hamilton, B.; Ogungbe, O.; Page II, R.L.; Rezk-Hanna, M.; Robertson, R.M.; Whitsel, L.P. on behalf of the American Heart Association Advocacy Coordinating Committee (2025). Impact of Smokeless Oral Nicotine Products on Cardiovascular Disease: Implications for Policy, Prevention, and Treatment: A Policy Statement From the American Heart Association. Circulation 151(1):e1-e21. https://doi.org/10.1161/CIR.0000000000001293.
Benowitz, N.L. (2009). Pharmacology of Nicotine: Addiction, Smoking-Induced Disease, and Therapeutics. Annual Reviews of Pharmacological Toxicology 49:57-71. doi:10.1146/annurev.pharmtox.48.113006.094742.
Carlsson, S.; Andersson, Aragh, M.; Galanti, R.; Lager, A.; Lundberg, M.; Nilsson, P.; Norberg, M.; Pedersen, N.L.; Trolle-Lagerros, Y.; Magnusson, C. (2017). Smokeless tobacco (snus) is associated with an increased risk of type 2 diabetes: results from five pooled cohorts. Journal of Internal Medicine 281:398-406. doi:10.1111/joim.12592.
Fisher, M.A.; Taylor, G.W.; Tilashalski, KR. (2005). Smokeless tobacco and severe active periodontal disease. NHANES III. J. Dent. Res. 84:705-10.
Gudnadottir, A.Y.; Olafsdottir, I.S.; Middelveld, R.; Ekerljung, L.; Forsberg, B.; Franklin, K.; Lindberg, E.; Janson, C. (2017). An investigation on the use of snus and its association with respiratory and sleep-related symptoms: a cross-sectional population study. BMJ Open 7:e15486. doi:10.1136/bmjopen-2016-015486.
Hajat, C.; Stein, E.; Ramstrom, L.; Shantikumar, S.; Polosa, R. (2021). The health impact of smokeless tobacco products: a systematic review. Human Reduction Journal 18:123. https://doi.org/10.1186/s12954-021-00557-6.
Yaddai, S.S.; Mohammed, M.M.; Abdelhakim, A.A.; Badrkhan, M.H.; Emam, A.A.I.; Alshatti, A., Shetty, R.M. (2024). The prevalence of Smokeless Tobacco Consumption and Its Effects on Gingival and Periodontal Health Among the Adults in the Emirates of Sharjah, UAE — A Cross-Sectional Study. Journal of Pharmacy and Bioallied Sciences 16:S1447-52.
Yang, F.; Pedersen, N.L.; Ye, W.; Liu, Z.; Norberg, M.; Forsgren, L.; Lagerros, Y.T.; Bellocco, R.; Alfredsson, L.; Knutsson, A.; Jansson, J-H; Wennberg, P.; Galanti, M.R.; Lager, A.C.J.; Aragh, M.; Lundberg, M.; Magnusson, C.; Wirdefelt, K. (2017). Moist smokeless tobacco (Snus) use and risk of Parkinson’s disease. Int J Epidemiol. 46(3):872-880. doi:10.1093/ije/dyw294.


